The Wall Street Journal reports that
Lawmakers raced to put finishing touches on a roughly $900 billion coronavirus aid package, pushing up against a midnight deadline to complete the agreement and pass it through Congress.
With a disagreement on the Federal Reserve’s emergency lending powers settled earlier in the weekend, negotiators on Sunday were finalizing details for the rest of the bill. Senate Majority Leader Mitch McConnell (R., Ky.) said Sunday afternoon that negotiators were hours away from completing the deal. * * *
The emerging agreement is expected to provide $300 a week in enhanced federal unemployment benefits, a $600 direct check to many Americans, as well as aid for schools, vaccine distribution and small businesses. Final votes in the House and Senate could occur as early as Sunday.
Lawmakers raced to put finishing touches on a roughly $900 billion coronavirus aid package, pushing up against a midnight deadline to complete the agreement and pass it through Congress.
With a disagreement on the Federal Reserve’s emergency lending powers settled earlier in the weekend, negotiators on Sunday were finalizing details for the rest of the bill. Senate Majority Leader Mitch McConnell (R., Ky.) said Sunday afternoon that negotiators were hours away from completing the deal. * * *
The emerging agreement is expected to provide $300 a week in enhanced federal unemployment benefits, a $600 direct check to many Americans, as well as aid for schools, vaccine distribution and small businesses. Final votes in the House and Senate could occur as early as Sunday.
The House is expected to vote on a 24-hour extension of government funding Sunday evening, setting up votes on the relief agreement and broader spending bill for Monday. The aid package is tied to a roughly $1.4 trillion annual spending package and Congress has passed a series of temporary spending bills in recent days to keep the government funded while it finished the negotiations.
Significantly, Politico reports that “Congress is set to include a long-elusive ban on “surprise” medical bills as part of a major spending deal lawmakers were working to finalize Sunday evening.”
(P.S. Govexec.com confirms that Congress passed a one day extension of the continuing resolution Sunday night.)
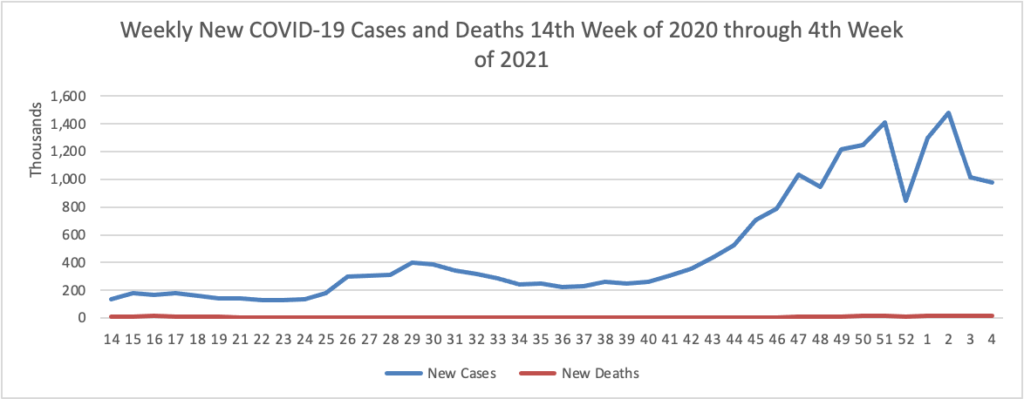
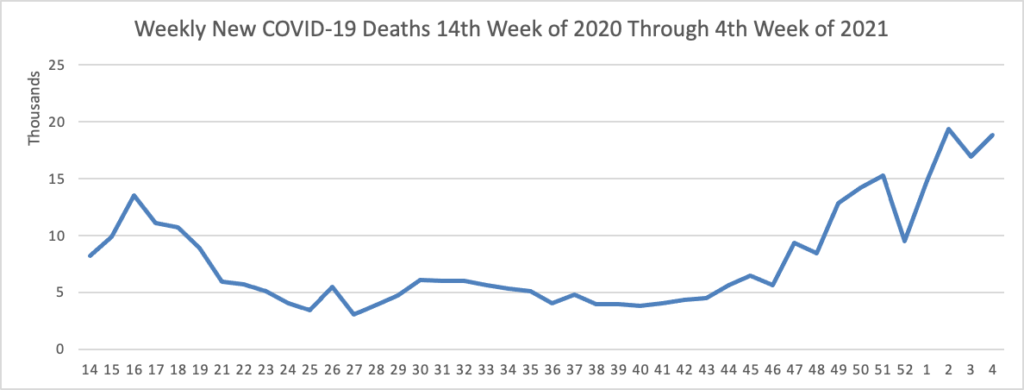
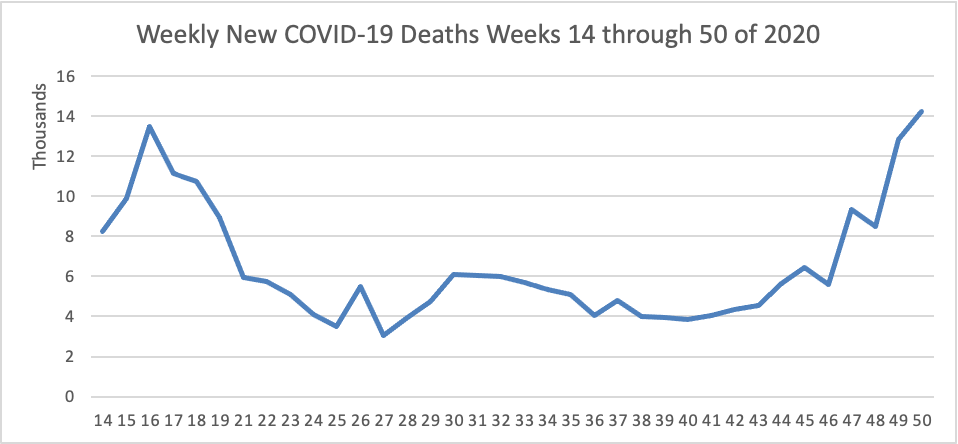
On the COVID-19 front —
The Centers for Disease Control now has a COVID-19 vaccines website which indicates that as of 1 pm today 2,838,225 doses of vaccine have been distributed and 556,208 doses have been administered in the first week.
In accordance with CDC Advisory Committee on Immunization Practices recommendations, the current phase 1A of distribution is directed at healthcare personal and nursing home residents, The Wall Street Journal reports that ACIP today approved phases 1B and 1C as follows:
The next group would include people ages 75 and older, whose hospitalization and death rates are the highest of all age groups. It would also include teachers, factory workers, police and firefighters, grocery store workers and others who are considered essential to the functioning of the economy and at high risk of exposure to Covid-19.
Another group would follow them, comprised of people between the ages of 65 and 74, anyone age 16 or over with a medical condition that puts them at high risk of complications from Covid-19, and other essential workers. They include people who work in transportation and logistics, food service, water and wastewater, and energy sectors.
The ACIP vote was 13-1. State governors are the ultimate decision makers in their states but the FEHBlog understands the governors generally defer to ACIP. As the FEHBlog has noted the vaccines are being directly distributed to federal agencies too.
On the COVID-19 treatment front, the Wall Street Journal reports that
Doctors are treating a new flood of critically ill coronavirus patients with treatments from before the pandemic, to keep more patients alive and send them home sooner.
Last spring, with less known about the disease, doctors often pre-emptively put patients on ventilators or gave powerful sedatives largely abandoned in recent years. The aim was to save the seriously ill and protect hospital staff from Covid-19.
Now hospital treatment for the most critically looks more like it did before the pandemic. Doctors hold off longer before placing patients on ventilators. Patients get less powerful sedatives, with doctors checking more frequently to see if they can halt the drugs entirely and dialing back how much air ventilators push into patients’ lungs with each breath.
“Let us go back to basics,” said Dr. Eduardo Oliveira, executive medical director for critical-care services for AdventHealth Central Florida, which recommends its doctors stick with pre-pandemic guidelines for ventilator use. “The less you deviate from it, the better.”
Advances also include new drugs, most notably steroids, for severely ill patients.
In other healthcare news, Health Payer Intelligence informs us that
Payers may consider promoting ambulatory surgery centers as the ideal site of care for joint replacement surgeries, UnitedHealth Group’s recent research findings suggested.
“Findings from new UnitedHealth Group research underscore the importance of optimizing sites of care to improve patient safety and reduce costs,” the report summarized.
The study analyzed data 2018 and 2019 procedures conducted at Optum’s ambulatory surgery centers. The researchers used low- and medium-severity surgeries to from the baseline and gauge shifts in costs and savings. They used the Ambulatory Surgery Centers Quality Collaboration’s recommended outcome measures to assess quality of care.
On the SolarWinds backdoor hack front, check out this ArsTechnica article:
Of the 18,000 organizations that downloaded a backdoored version of software from SolarWinds, the tiniest of slivers—possibly as small as 0.2 percent—received a follow-on hack that used the backdoor to install a second-stage payload. The largest populations receiving stage two were, in order, tech companies, government agencies, and think tanks/NGOs. The vast majority—80 percent—of these 40 chosen ones were located in the US.
These figures were provided in an update from Microsoft President Brad Smith. Smith also shared some insightful and sobering commentary on the significance of this almost unprecedented attack. His numbers are incomplete, since Microsoft sees only what its Windows Defender app detects. Still, Microsoft sees a lot, so any difference with actual numbers is likely a rounding error.
The FEHBlog had been wondering why not all of the victims of the backdoor hack were breached. It was a conscious decision by the hackers.