The New York Times reports that “The Food and Drug Administration warned on Monday that Johnson & Johnson’s coronavirus vaccine can lead to an increased risk of a rare neurological condition known as Guillain–Barré syndrome, another setback for a [one dose] vaccine that has largely been sidelined in the United States. Although regulators have found that the chances of developing the condition are low, they appear to be three to five times higher among recipients of the Johnson & Johnson vaccine than among the general population in the United States, according to people familiar with the decision. The warning was attached to factsheets about the vaccine for providers and patients.”
USA Today offers a success story on AHIP’s Vaccine Community Connectors program. “Most important, this effort helped the industry home in on one specific strategy to accelerate health equity: better access to health care data that incorporates the social determinants of health.” Speaking SDOH data, Health IT Analytics informs us about the use of SDOH data in researching and managing Alzheimer’s Disease.
The American Hospital Association reminded folks today to keep its Vaccine Communications Resources website in mind.
“The Biden administration has started to investigate whether Medicare should cover the extremely pricey Alzheimer’s drug aducanumab. The Centers for Medicare & Medicaid Services announced Monday it is opening a National Coverage Determination (NCD) analysis on the drug that will cost patients $56,000 a year. Advocates and experts have called for the agency to move quickly to decide whether to cover the drug. “We want to consider Medicare coverage of new treatments very carefully in light of the evidence available,” said CMS Administrator Chiquita Brooks-LaSure, in a statement Monday. “That’s why our process will include opportunities to hear from many stakeholders.”
Earlier press reports on Aduhelm, as well as common sense, indicate that commercial health plans likely will follow CMS’s lead on coverage of that drug.
Healthcare Dive tells us that “Telehealth use overall has stabilized at levels 38 times higher than before the COVID-19 pandemic, ranging from 13% to 17% of visits across all specialties, according to new data from McKinsey released roughly a year since the first major spike in COVID-19 cases.” * * * On the provider side, 58% of physicians continue to view virtual care more favorably than before the pandemic, though that’s down slightly from September, when 64% of physicians were in support. As of April this year, 84% of doctors were offering telehealth, and 57% said they’d prefer to continue offering it. However, that’s largely dependent on reimbursement: 54% of doctors said they wouldn’t provide virtual care if it was paid at a 15% discount to physical services.”
HR Dive discusses the President’s July 9 executive order provision “taking aim at” non-compete agreements.
Biden’s order leaves some questions unanswered. It does not ban or impact any existing employment agreement, Chris Marquardt, partner at Alston & Bird, told HR Dive in an email. “Employers will need to wait and see what the Federal Trade Commission does in response to the Executive Order before thinking about its potential impact,” he said.
Among other reasons, intellectual property and trade secrets have been cited as cause for use of non-competes. But the agreements have been the subject of criticism for potentially driving down wages in certain industries and geographic areas.
Govexec.com offers an interesting take on how the July 9 executive order seeks to use Federal procurement and regulations to promote competition
This coming week, the House of Representatives resumes Committee business and the Senate resumes both Committee business and floor voting. The Wall Street Journal adds that “After a two-week recess, senators return to Washington this week to determine the fate of much of President Biden’s roughly $4 trillion agenda. Senate Majority Leader Chuck Schumer (D., N.Y.) told Senate Democrats in a letter on Friday that he expects that the chamber will take up both a roughly $1 trillion infrastructure agreement and a resolution setting the parameters of a bill encompassing other Democratic priorities in the coming weeks.”
Returning to the President’s July 9, 2021, executive order on competition the accompanying Fact Sheet explains that with regard to healthcare:
BEGIN QUOTE
In the Order, the President:
Directs the Food and Drug Administration to work with states and tribes to safely import prescription drugs from Canada, pursuant to the Medicare Modernization Act of 2003.
Directs the Health and Human Services Administration (HHS) to increase support for generic and biosimilar drugs, which provide low-cost options for patients.
Directs HHS to issue a comprehensive plan within 45 days to combat high prescription drug prices and price gouging.
Encourages the FTC to ban “pay for delay” and similar agreements by rule.
Hearing Aids: Hearing aids are so expensive that only 14% of the approximately 48 million Americans with hearing loss use them. On average, they cost more than $5,000 per pair, and those costs are often not covered by health insurance. A major driver of the expense is that consumers must get them from a doctor or a specialist, even though experts agree that medical evaluation is not necessary. Rather, this requirement serves only as red tape and a barrier to more companies selling hearing aids. The four largest hearing aid manufacturers now control 84% of the market. In 2017, Congress passed a bipartisan proposal to allow hearing aids to be sold over the counter. However, the Trump Administration Food and Drug Administration failed to issue the necessary rules that would actually allow hearing aids to be sold over the counter, leaving millions of Americans without low-cost options.
In the Order, the President:
Directs HHS to consider issuing proposed rules within 120 days for allowing hearing aids to be sold over the counter.
Hospitals: Hospital consolidation has left many areas, especially rural communities, without good options for convenient and affordable healthcare service. Thanks to unchecked mergers, the ten largest healthcare systems now control a quarter of the market. Since 2010, 139 rural hospitals have shuttered, including a high of 19 last year, in the middle of a healthcare crisis. Research shows that hospitals in consolidated markets charge far higher prices than hospitals in markets with several competitors.
In the Order, the President:
Underscores that hospital mergers can be harmful to patients and encourages the Justice Department and FTC to review and revise their merger guidelines to ensure patients are not harmed by such mergers.
Directs HHS to support existing hospital price transparency rules and to finish implementing bipartisan federal legislation to address surprise hospital billing.
Health Insurance: Consolidation in the health insurance industry has meant that many consumers have little choice when it comes to selecting insurers. And even when there is some choice, comparison shopping is hard because plans offered on the exchanges are complicated—with different services covered or different deductibles.
In the Order, the President:
Directs HHS to standardize plan options in the National Health Insurance Marketplace so people can comparison shop more easily.
END QUOTE
Roll Call and Healthcare Dive relate industry reaction to the order. The FEHBlog is not happy with drug importation from Canada directive because our population exceeds Canada’s by ten times. It’s a gimmic. Also the FEHBlog disagrees with standardizing plan designs which by definition inhibits competition. Also the objections to hospital and health insurer consolidation overlooks the fact that the Affordable Care Act largely has driven the consolidation, in the FEHBlog’s opinion.
The Health Affairs Blog discusses Centers for Medicare Services efforts to keep its Medicare Part B schedule current. The article explains
Currently, physician services in the US are priced by Medicare every January 1 in relative value units (RVUs). Every physician service is assigned a Medicare-allowed price in RVUs based on its work “intensity” defined by time, effort, skill, and stress relative to all other services. RVUs are converted to dollars via the Medicare “conversion factor,” which CMS sets annually. Total Medicare allowed payment for each service also includes RVUs for practice expenses and malpractice risk, which are theoretically unrelated to physician compensation.
Commercial insurers generally use the same RVU fee schedule as the basis for physician payments. Value-based payment models use Medicare valuations for calculating costs and payments.
In recent decades, technological advances have substantially expanded the number of procedural services, which are generally priced far above evaluation and management (E/M) services. As procedures are increasingly completed safely in less time, the RVU generation potential of procedurally oriented physician work has also grown. In contrast, the analogous expansion of therapeutic choices and medications that are at the core of E/M services have not been reflected by increased valuations. This has contributed to widened income gaps between proceduralists and non-proceduralists, leading to the lack of incentives for trainees to enter lower-reimbursed specialties, including primary care, endocrinology, oncology, rheumatology, and infectious diseases.
After a slower January and February, federal retirement seems to be picking back up in the first half of 2021 compared to 2020. June stats from the Office of Personnel Management for newly filed claims showed last month was higher than a year ago, when the pandemic was in full effect.
OPM received 7,264 new retirement claims last month compared to 6,555 new claims in June 2020 — a 10.8% increase. March, April and May each saw year-over-year increases ranging from 15.6%- 47.2%.
Processing them all is a different matter, as last month saw 6,884 claims processed compared to 7,300 processed in June 2020 — a 5.7% decrease. After peaking in March, the claims backlog has been moving downward, but at 24,999 last month is still 30.3% higher than a year ago and 92.3% higher than the steady state goal of 13,000 claims — nearly double.
From the COVID-19 front, Bloomberg informs us that “In the U.S., 334 million doses have been given so far. In the last week, an average of 506,771 doses per day were administered.” According to the CDC, 159.3 million Americans are fully vaccinated. The Wall Street Journal adds that “[While] millions of Americans have rolled up their sleeves to get vaccinated against Covid-19, one group is well behind: young adults.
Their reluctance is a significant part of why the U.S. missed the Biden administration’s goal of getting 70% of the adult population a first dose by July 4, and it is impeding efforts to develop the communitywide immunity sought to move past the pandemic and fend off Delta and other variants.
Now government health authorities are dialing up efforts encouraging 18- to 29-year-olds to get vaccinated.
Turning to the telehealth front,
The American Medical Association provides tips on how physicians can being warmth to the virtual visit.
Healio informs us that “New research suggests a letter may be all that it takes to lower the number of telehealth no-shows among older patients, even during a pandemic. * * * ‘The letter was a very simple reminder, stating ‘You have an upcoming telehealth visit with your doctor’ and included the date and a range of time that the provider would call, typically a 30-minute period,’ [researcher / physician Sarah] King said in the interview. * * * Overall, the researchers said their intervention was associated with a 33.1% drop in the telehealth no-show rate and an 8% drop in the no-show rate for in-person visits.”
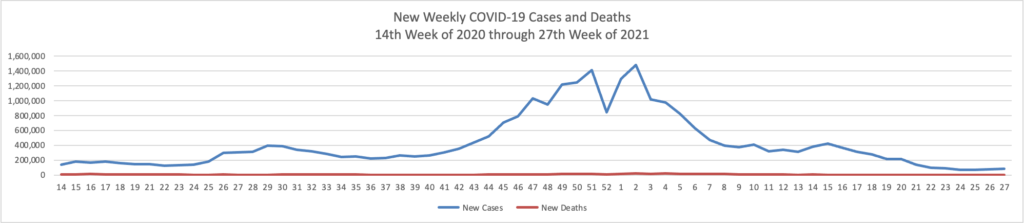
Based on the Centers for Disease Control’s COVID-19 Data Tracker website, here is the FEHBlog’s chart of new weekly COVID-19 cases and deaths over the 14th week of 2020 through 27th week of this year (beginning April 2, 2020, and ending July 7, 2021; using Thursday as the first day of the week in order to facilitate this weekly update):
and here is the CDC’s latest overall weekly hospitalization rate chart for COVID-19:
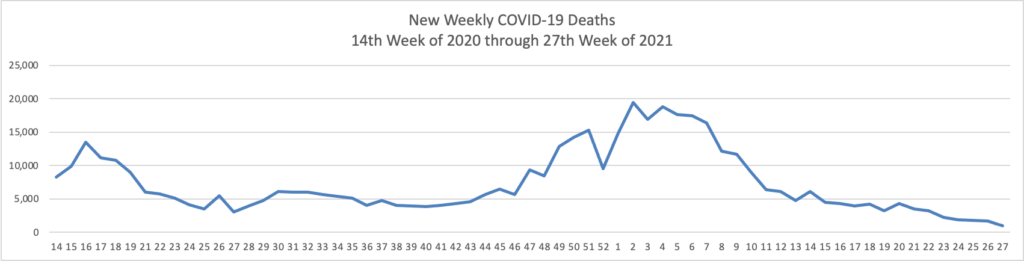
The FEHBlog has noticed that the new cases and deaths chart shows a flat line for new weekly deaths because new cases significantly exceed new deaths. Accordingly here is a chart of new COVID-19 deaths over the period (April 2, 2020, through July 7, 2021):
This is the first week since the FEHBlog began the chart that the number of new weekly deaths (955) has fallen below 1,000 nationwide.
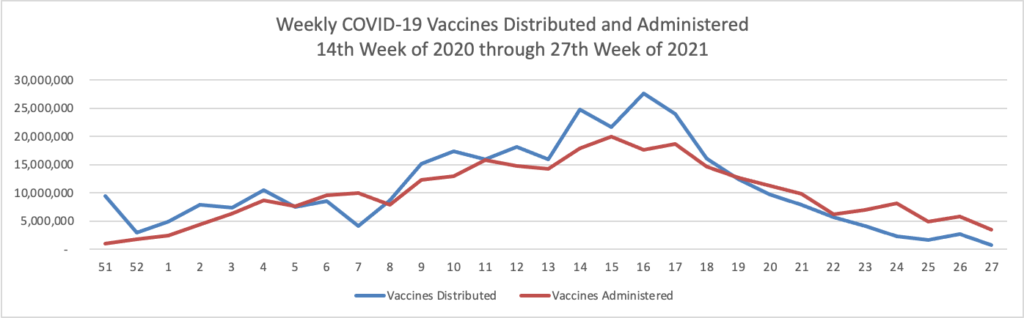
Finally here is a COVID-19 vaccinations chart over the period December 17, 2020, through July 7, 2021 which also uses Thursday as the first day of the week:
The Centers for Disease Control reports that “The COVID Data Tracker Vaccination Demographic Trends tab shows vaccination trends by age group. As of July 8, 88.5% of people ages 65 or older have received at least one dose of vaccine and 78.8% are fully vaccinated. Just over two-thirds (67.3%) of people ages 18 or older have received at least one dose of vaccine and 58.5% are fully vaccinated. For people ages 12 or older, 64.5% have received at least one dose of vaccine and 55.8% are fully vaccinated.”
Today, the President issued a wide ranging executive order on promoting competition in the American economy, which of course had been humming along nicely before the pandemic struck. Here’s a link to the fact sheet on the executive order which recounts its 70+ initiatives. The FEHBlog call attention to several healthcare initiatives in Sunday’s posts. The FEHBlog sense that this executive order will generate a lot of litigation.
The Food and Drug Administration’s acting commissioner, Janet Woodcock, is taking the highly unusual step of asking for a federal investigation of doctors within her own agency who met with the makers of an Alzheimer’s drug before the medicine’s recent approval.
Dr. Woodcock, in a letter made public Friday, called for the Office of Inspector General of the Department of Health and Human Services, which oversees the FDA, to review interactions between the drugmaker [Biogen] and FDA staff during the approval process.
The drug’s approval has been highly controversial, partly because of its annual price pegged at $56,000, and partly because evidence of the drug’s effectiveness was inconclusive.
This unusual step certainly will make the FDA decision makers think twice before crossing their advisory committee again. Biogen added fuel to the fire with its outrageous pricing.
Fierce Healthcare reports that “The quick rollout of the COVID-19 vaccine in the U.S. saved an estimated 279,000 lives and prevented 1.25 million hospitalizations, a new study finds. The study, released Wednesday, warns, however, that surges of new cases due to the highly transmissible delta variant could reverse these gains. “Until a greater majority of Americans are vaccinated, many more people could still die from this virus,” said Alison Galvani, Ph.D., director of the Yale Center for Infectious Disease Modeling and Analysis, which conducted the study alongside the Commonwealth Fund.”
The Wall Street Journal reports that “Children are at extremely slim risk of dying from Covid-19, according to some of the most comprehensive studies to date, which indicate the threat might be even lower than previously thought. Some 99.995% of the 469,982 children in England who were infected during the year examined by researchers survived, one study found. In fact, there were fewer deaths among children due to the virus than initially suspected. Among the 61 child deaths linked to a positive Covid-19 test in England, 25 were actually caused by the illness, the study found.”
The Journal also informs us that “Pfizer Inc. will seek clearance from U.S. regulators in coming weeks to distribute a booster shot of its Covid-19 vaccine to heighten protection against infections as new virus strains rise. The company said also it plans to start clinical trials in August of an updated version of its vaccine that would better protect against the Delta variant.” While the FEHBlog looks forward to lining up for the booster, Axios reports that “People who are fully vaccinated against the coronavirus do not need a booster shot at this time, the Food and Drug Administration and the Centers for Disease Control and Prevention said in a joint statement released Thursday evening.” Axios adds
One dose of the Pfizer-BioNTech or AstraZeneca coronavirus vaccine “barely” protects against the Delta variant of the virus, because of mutations the variant has developed, a new study published in the journal Nature Thursday found.
But two doses of those vaccines generated a neutralizing response to the variant in 95% of people, highlighting the importance of full vaccination against COVID-19, Axios’ Jacob Knutson writes.
Bloomberg discusses the idea of offering COVID-19 vaccines at Dollar General stores. “The researchers found that in the most vulnerable decile, the number of retail pharmacies that are eligible to provide vaccines through the Federal Retail Pharmacy Program is the lowest. But these vulnerable regions are also where Dollar General and other discount stores like it tend to cluster.” It’s worth a shot?
The National Institutes of Health released its annual joint report on cancer mortality. “The report shows a decrease in death rates for 11 of the 19 most common cancers among men, and for 14 of the 20 most common cancers among women, over the most recent period (2014-2018). Although declining trends in death rates accelerated for lung cancer and melanoma over this period, previous declining trends for colorectal and female breast cancer death rates slowed and those for prostate cancer leveled off. Death rates increased for a few cancers like brain and other nervous system and pancreas in both sexes, oral cavity and pharynx in males, and liver and uterus in females.” STAT News points out
Accelerating declines in lung cancer deaths may account for much of the overall progress seen in recent years, the authors of the report said. Over the past two decades, the death rate for lung cancer has declined even faster than the rate at which patients are diagnosed with the disease. And while part of the early success in preventing lung cancer can be attributed to the massive drop in smoking rates, the authors note the most recent downward trends seem to correspond with the approval of new treatments for non-small cell lung cancer that improved the likelihood of survival.
Death rates from melanoma also saw an accelerated decline in the past decade, despite a growing number of diagnoses. Like in lung cancer, authors point to the introduction of novel treatments around the same time as the turnaround on the death rate. New targeted and immune checkpoint inhibitors were approved by the Food and Drug Administration in 2011, one year before major declines in death rates were seen in women and two years before they were seen in men.
On the prescription drug front
The New York Times reports that “Under fire for approving a questionable drug for all Alzheimer’s patients, the Food and Drug Administration on Thursday greatly narrowed its previous recommendation and is now suggesting that only those with mild memory or thinking problems should receive it. The reversal, highly unusual for a drug that has been available for only a few weeks, is likely to reduce the approximate number of Americans who are eligible for the treatment to 1.5 million from six million.”
GoodRX points out and discusses the fifteen most addictive prescription drugs and resource available to help the addicted. The National Institute on Drug Abuse has an outreach website for teenagers, for example.
In other healthcare news
Health Affairs blog bangs the drum for Congress to fund a universal patient identifier. For the reasons explained in the article, this step called for in the HIPAA statute of 1996 is long overdue.
Healthcare Dive reports that “Telehealth claim lines as a percentage of all medical claims dropped 13% in April, marking the third straight month of declines, according to new data from nonprofit Fair Health. The dip was greater than the drop of 5.1% in March, but not as large as the decrease of almost 16% in February. However, overall utilization remains significantly higher than pre-COVID-19 levels. The decline appears to be driven by a rebound in in-person services, researchers said. Mental health conditions bucked the trend, however, as the percentage of telehealth claim lines associated with mental conditions — the No. 1 telehealth diagnosis — continued to rise nationally and in every U.S. region.” The FEHBlog considers that to be good news because telehealth at least currently is best suited for mental health care and out of schedule healthcare situations.
In closing, the FEHBlog wants to emphasize an important aspect of last Thursday’s No Surprise Billing rule. As explained in the government’s model consumer notice for use by health plans,
When you get services from an in-network hospital or ambulatory surgical center, certain providers there may be out-of-network. In these cases, the most those providers may bill you is your plan’s in-network cost-sharing amount. This applies to emergency medicine, anesthesia, pathology, radiology, laboratory, neonatology, assistant surgeon, hospitalist, or intensivist services. These providers can’t balance bill you and may not ask you to give up your protections not to be balance billed.
If you get other services at these in-network facilities, out-of-network providers can’t balance bill you, unless you give written consent and give up your protections.”
The vast majority of surprise bills stem from out-of-network service provided by emergency rooms, air ambulance, and the types of providers listed above, all of whom are locked into using negotiation and baseball arbitration with the health plan. The only doctors who can approach the patient for a balancing billing waiver are the surgeon or oncologist in a non-emergency setting who meets with the patient well before the surgery. That makes sense.
This approach, however, will promote use of the independent dispute resolution system which the tri-agencies will unveil October 1. Three months is more than ample time for the FEHBlog’s fellow lawyer to prepare for this new business opportunity. Health plans should make sure that their out of network pricing negotiators are adequately staffed.
The Wall Street Journal reports that “The highly transmissible Delta variant has become the dominant strain of the Covid-19 virus circulating in the U.S., according to federal data. It is spreading rapidly as communities loosen pandemic restrictions and officials struggle to reach unvaccinated people. The Delta variant, also known as B.1.617.2, made up 51.7% of Covid-19 infections in the two weeks ended July 3, according to genetic sequences from positive Covid-19 tests submitted to the U.S. Centers for Disease Control and Prevention.”
The Journal adds that “Covid-19 vaccines available in the U.S. protect against the Delta variant, but the virus is of great risk to people who aren’t vaccinated, according to public-health and infectious-disease experts. * * * Warm weather is helping to keep numbers of new cases down, and infections are likely to rise again in the fall, said Dr. Paul Sax, clinical director of the Division of Infectious Diseases at Brigham and Women’s Hospital in Boston. ‘Last summer we got a little bit overconfident,’ he said. ‘I don’t want us to make the same mistake again this time. We need to push as hard as we can to get as many people vaccinated as possible.’”
AHIP updates us on the progress made by its Vaccination Community Connectors program. “The COVID-19 pandemic has been a fundamental part of Americans’ lives for 15 months and counting. America cannot afford to lose any more time in achieving community immunity. Public-private partnerships have helped to support our communities through the crisis this far. By extending those partnerships through secure sharing of data about who has been immunized, we can better target every outreach and connection to put an end to the pandemic and get back to the moments we all miss. For more information, read our white paper with Blue Cross Blue Shield Association (BCBSA) and the Association for Community Affiliated Plans (ACAP).”
The FEHBlog noticed today that the OPM Inspector General has posted his semi-annual report to Congress for the period ended April 30, 2021, and OPM’s management response thereto. The Inspector General’s report includes an update of his earlier assessment of the pandemic’s impact on the FEHB Program. With all due respect, the FEHBlog finds the OIG’s assessment unnecessarily pessimistic but it’s for the readers to form their own opinions.
From the innovation front
Fierce Pharma reports that “Many pursuits have been put on hold during the coronavirus pandemic. But biopharmaceutical innovation isn’t one of them. In 2020, the FDA approved 53 new drugs, the second-most in a single year, after 2018’s bounty of 59. And the momentum has continued through the first half of 2021. With the FDA endorsing its 29th novel drug on June 30, the industry was slightly ahead of last year’s pace. * * * n terms of treatment areas, it is of little surprise that oncology accounts for 12 of this year’s approvals. That figure represents 44% of all new drug approvals this year, an even higher rate than in 2020 when 20 of 53 new drugs were in the oncology class. * * * The FDA’s roundups of 2021’s novel drug approvals can be found here and here.”
Employee Benefit News informs us that “Employers have a new tool in their arsenal to help employees reach a healthier weight and reduce their healthcare costs. DayTwo, a precision medicine company, has released new outcomes from its employer and health plan nutrition programs, to tackle high-risk and high-cost metabolic conditions, like obesity, Type 2 diabetes and pre-diabetes. The program provides users with a microbiome screening, which measures how the body digests food, in order to offer AI-powered nutritional plans tailored to their needs. After one year, employees who used the DayTwo program lost an average of 19 pounds and reduced their body mass index by 3.3 points, according to a release. The program is meant to reduce the reliance on medication and help employees with obesity and Type 2 diabetes lose weight naturally.”
mHealthIntelligence tells us that “While many healthcare providers are just now getting into the remote patient monitoring arena, Ochsner Health has scaled its platform to a national level, and is now monitoring more than 20,000 people in health plans across the country. And still, says Julie Henry chief operating officer for the New Orleans-based health system’s digital medicine department, ‘we’re learning lessons each and every day.’ That’s one of the guiding principles behind a connected health service that is seeing immense growth in the wake of the coronavirus pandemic, which has pushed many health systems to shift healthcare services from the hospital to the home. It’s a work in progress for everyone, from those deploying the technology to those paying for it. And there isn’t a hospital, clinic or practice out there that isn’t learning something new.”
In other healthcare news
The Federal Register announced today the last Thursday’s No Surprises Act interim final rule will be published in the July 13 issue. Publication triggers the sixty day public comment period which should end on Monday September 13 (as the 60 day period ends on Saturday September 11.)
Beckers Hospital Review reports that “Amazon Care, the e-commerce giant’s new healthcare venture, has approached several big health insurers in an effort to expand coverage of its services, Insider reported July 7. The healthcare venture reportedly talked to Aetna, Premera Blue Cross and Blue Cross Blue Shield of Massachusetts, according to people familiar with the discussions.”
The Hill informs us that “President Biden on Tuesday pleaded with Americans to get vaccinated against COVID-19 as the White House signaled a shift toward grassroots tactics to reach those who have yet to get a shot.” Here is a link to the President’s full remarks.
NPR Shots offers a daily look at each state’s progress in vaccinating its residents.
From the hospital pricing transparency front —
The Wall Street Journal explains how it has been analyzing the pricing data that federal law required hospitals to make publicly available on January 1, 2021. “The Journal reviewed hospital pricing disclosures collected by Turquoise Health Co., a startup that has been gathering the data from hospital websites since the regulations went into effect.” The Turquoise Health website is worth a gander.
NPR Shots also analyzed the newly available hospital pricing data. “While it’s still an unanswered question about whether price transparency will lead to overall lower prices, KHN took a dive into the initial trove of data to see what it reveals. Here are five takeaways from the newly public data and tips for how you might be able to use it to your benefit: 1) As expected prices are all over the map; 2. Patients can look up information but the info is incomplete; 3. Third party firms like Turquoise Health are trying to make searching prices simpler and cash in; 4. Consumers can use the data to negotiate with hospitals when paying cash, and 5. Hospitals are not fully on board currently.
In the tidbits department —
Today, the Centers for Medicare and Medicaid Services announced Dr. Meena Seshamani, M.D., Ph.D. [formerly with MedStar Health] as Deputy Administrator and Director of Center for Medicare. She started her work today.
Fierce Healthcare reports “The United Health Foundation, the philanthropic arm of the UnitedHealth Group, released its America’s Health Rankings Health Disparities Report last week, and the healthcare giant found a number of disparities worsened in the 2017 to 2019 time frame. While the data come from before the pandemic, experts say they offer a baseline that can be used to address critical public health needs. For example, adults who did not graduate high school had a rate of frequent mental distress that was 123% higher than people with a college degree. Females had a 70% higher rate of depression than males, according to the report.”
NPR Shots discusses how an “obesity drug’s [Wegovy] promise now hinges on insurance coverage.”
In clinical trials, weekly injections of semaglutide — or Wegovy, as it’s been branded —helped people drop an average of 15% of their body weight. That’s an average of about 34 pounds over 16 months, before their weight plateaued, a far greater weight loss, obesity specialists say, than achieved with other drugs on the market. At least as important, Wegovy raised none of the alarm bells with the FDA or obesity doctors that it might trigger serious side effects of the sort some people experienced by taking fen-phen or other previous medical treatments for obesity.
But with a price tag for Wegovy of $1,000 to $1,500 a month, a big question remains: Will insurers cover its significant cost for the millions who might benefit? * * *
Insurance coverage, it turns out, is a giant question — not just with Wegovy but with obesity drugs in general. Some private insurers do include some prescription obesity drugs in the list of medicines they’ll cover; it’s too early to tell whether Wegovy will make those lists. Many doctors and patients are optimistic, because it is a higher dose of an existing diabetes medication called Ozempic, which insurers often cover.
A few select state Medicaid programs will cover medications that treat obesity in some circumstances. But, significantly, Medicare does not cover obesity drugs — and many private insurers typically follow Medicare’s lead.
Yet the demand for a good treatment is there, says Dr. Fatima Cody Stanford, a leading obesity researcher at Harvard. She was not involved in conducting the Wegovy clinical trial but closely followed it. “I’m excited about it,” she says, because of the dramatic weight loss.
The drug acts on the brain so people eat less and store less of what they eat. That helps address the excess weight as well as helping with related diseases of the liver or heart, for example.
The FEHBlog enjoys book recommendations and so he lapped up STAT’s list of “the 36 best books and podcasts on health and science to check out this summer. Among them, this one particularly caught the FEHBlog’s attention as he has enjoyed reading this author’s output and the topic is intriguing: “The Code Breaker: Jennifer Doudna, Gene Editing, and the Future of the Human Race”By Walter Issacson I recommend it because this captivating book provided clear and accessible explanations of the scientific discovery of CRISPR-Cas9 and its remarkable power as a gene editing tool, interwoven with the complex human stories of Jennifer Doudna and her relationships with the many other accomplished scientists who brought it all together.— Anthony Fauci, director of the National Institute of Allergy and Infectious Diseases”
The federal regulators, including the Office of Personnel Management, achieved their statutory deadline today for issuing the first round of No Surprises Act implementing rules. Here’s the regulators’ output, compliments of the Labor Department:
There is no doubt in the FEHBlog’s mind that the regulators did a fine job of making a silk purse out of sow’s ear / the poorly drafted statute. This rule will help carriers and providers meet the January 1, 2022, launch date. This law, if properly implemented, and signs are looking good now, will protect consumers from surprise medical bills, which was clearly Congress’s objective, but without creating an IT nightmare.
The regulators plan a second round of No Surprises Act rules for October 1, 2021. The second round will focus on the independent dispute resolution process.
From the COVID-19 front —
The New York Times reports that “The Johnson & Johnson coronavirus vaccine is effective against the highly contagious Delta variant, even eight months after inoculation, the company reported on Thursday — a finding that should reassure the 11 million Americans who have gotten the shot. The vaccine showed a small drop in potency against the variant, compared with its effectiveness against the original virus, the company said. But the vaccine was more effective against the Delta variant than the Beta variant, first identified in South Africa — the pattern also seen with mRNA vaccines.”
Medscape informs us that “The White House on Thursday announced it will send “strike teams” to 1000 counties where the COVID-19 Delta variant is spreading rapidly. The teams will be made up of health and logistics experts from several federal agencies and will conduct coronavirus testing, distribute medicines designed to fight the virus, and boost local and state efforts to increase vaccinations.”
In Thursday Miscellany —
GoodRx is tracking prescription drug manufacturer price changes which typically are made effecting January 1 and July 1.
The Centers for Medicare and Medicaid Services “is proposing actions that aim to close health equity gaps by providing Medicare patients battling End-Stage Renal Disease (ESRD) with greater access to care, through the ESRD Prospective Payment System (PPS) annual rulemaking. This proposed rule would update ESRD PPS payment rates, make changes to the ESRD Quality Incentive Program (QIP), and modify the ESRD Treatment Choices (ETC) Model. The proposed changes to the ETC Model policies would aim to encourage dialysis providers to decrease disparities in rates of home dialysis and kidney transplants among ESRD patients with lower socioeconomic status, making the model the agency’s first CMS Innovation Center model to directly address health equity.”
The Aetna Foundation and U.S. News and World Report released their 2021 healthiest U.S. communities rankings this week.
Yesterday the House Appropriations Committee approved for House floor consideration the Fiscal Year 2022 Financial Services and General Government appropriations bill which includes OPM and FEHB Program funding. The vote was 33-24. Govexec adds that the Committee action “endorses President Biden’s proposal to give civilian federal employees an average 2.7% pay raise in 2022, despite efforts by some Democrats to provide a bigger increase.”
Amy Howe informs us that tomorrow will be the last day of the U.S. Supreme Court’s October 2020 term and the two remaining decisions are politically significant.
The Society for Human Resource Management reports that ”The Equal Employment Opportunity Commission (EEOC) has extended the deadline for filing the EEO-1 form from July 19 to Aug. 23. Businesses with 100 or more employees and some federal contractors with at least 50 employees must submit an annual EEO-1 form, which asks for information from the previous year about the number of employees who worked for the business, sorted by job category, race, ethnicity and gender. The EEOC did not collect such data in 2020 due to the coronavirus crisis. Covered employers now have until the new deadline to submit both their 2019 and 2020 data.”
The Office of Management and Budget’s Office of Information and Regulatory Affairs has completed its work on HHS’s first interim final rule on implementing the No Surprises Act. Next step will be the Federal Register’s public inspection list.
From the COVID-19 front
The Centers for Disease Control has improved its COVID-19 data tracker website. Check out this fascinating new chart on the value of the COVID-19 vaccines.
The Wall Street Journal reports that “People who became infected with Covid-19 after getting a messenger RNA vaccine [Pfizer or Moderna] carried less virus and had shorter cases than unvaccinated people who became infected, a study by government health researchers found. * * * “Even when people get vaccinated and did get infected, they were less likely to have an illness that causes a fever,” said Mark Thompson, an epidemiologist at the U.S. Centers for Disease Control and Prevention who helped lead the study.”
The American Hospital Association informs us that “The Moderna COVID-19 vaccine produces neutralizing antibody titers against the Delta variant, although fewer than against the ancestral strain of the virus, the company announced yesterday. * * * “These new data are encouraging and reinforce our belief that the Moderna COVID-19 Vaccine should remain protective against newly detected variants,” said CEO Stéphane Bancel.
From the Aduhelm front, STAT News tells us that A majority of U.S. physicians disagree with the Food and Drug Administration’s approval of the Alzheimer’s drug from Biogen (BIIB) and believe the medicine should not be routinely used, according to a new survey from STAT and Medscape. Nearly two-thirds of the 200 primary care physicians and neurologists polled find the trial data unclear when it comes to benefits and risks of the drug. Consequently, only a small minority of these doctors think the medicine should be given to patients with early-onset Alzheimer’s.
The controversial new Alzheimer’s drug would only be cost effective if priced between $3,000 and $8,400, an 85% to 95% discount off the $56,000 list price, due to “insufficient” evidence the drug benefits patients, STAT says, citing a revised analysis. The assessment by the Institute for Clinical and Economic Review is very similar to an evaluation issued a month ago, before the FDA approved the medicine and issued a broad label. But Biogen has pledged to promote the drug only to a more specific patient population and the FDA is requiring fewer costly MRI scans to monitor patient safety.
With regard to the physician survey and with all due respect to that fine profession, the FEHBlog expects that the “If you build it they will come” principle could apply to Aduhelm.
In other healthcare news
Barron’s reports that “The nation’s largest retailer is now selling the first private-label insulin at prices more than 50% lower than brand names of the diabetes drug, which can cost thousands of dollars a year. Walmart pharmacies began filling prescriptions this week for the discount chain’s ReliOn NovoLog brand of insulin in vials and injector pens. The drug, made by major supplier Novo Nordisk (NVO), will be available by mid-July at the company’s Sam’s Club wholesale stores. “We know many people with diabetes struggle to manage the financial burden of this condition, and we are focused on helping by providing affordable solutions,” Cheryl Pegus, executive vice president of Walmart Health & Wellness, announced Tuesday.”
Medscape informs us that “Families with private health insurance pay around $3,000 for newborn delivery and hospitalization, while adding neonatal intensive care can push the bill closer to $5,000, based on a retrospective look at almost 400,000 episodes. The findings suggest that privately insured families need prenatal financial counseling, as well as screening for financial hardship after delivery, reported lead author Kao-Ping Chua, MD, PhD, assistant professor and health policy researcher in the department of pediatrics and the Susan B. Meister Child Health Evaluation and Research Center at the University of Michigan, Ann Arbor, and colleagues. “Concern is growing regarding the high and rising financial burden of childbirth for privately insured families,” the investigators wrote in Pediatrics.” Health plans may want to take a gander at their own members out of pocket spending on maternity care.
The appeal of these companies has grown as employers increasingly seek to address a shortage of high-quality primary care and reduce spending on the health of their workforce, said Ellen Kelsay, CEO and president of the Business Group on Health, which represents large employers.
Studies show a strong correlation between access to primary care and lower spending on expensive medical services such as ER visits, surgeries and hospital admissions. Yet in the United States, primary care accounts for only around 5% to 7% of total health spending, compared with 14% in the 36 member nations of the Organization for Economic Cooperation and Development.
The big bet of One Medical and companies like it is that greater spending on primary care will fatten their bottom lines while reducing overall health costs for their clients. [One Medical works with health plans as well as self-funded employers and patients.]
Bloomberg has released its latest COVID-19 resilience ranking.
Almost a year and a half into the pandemic, the best and worst places to be in the Covid-19 era are increasingly defined by one thing: normalization.
The biggest vaccination drive in history is enabling parts of the globe to abolish mask mandates, relax restrictions and dismantle border curbs, making the magnitude of reopening key to quality of life. Taming cases and deaths was once paramount, along with ensuring a robust health-care system. Now, the ability to essentially turn back the clock and return to pre-pandemic times is taking on an even greater significance.
Central to that is an economy’s openness to the world, and that’s why we’ve introduced a new element—Reopening Progress—to Bloomberg’s Covid Resilience Ranking. Two new metrics capture the ease of moving in and out of a place and how much air travel has recovered, alongside our 10 other measures tracking mortality rates to infection counts, freedom of movement to economic growth.
This pivot has ushered in dramatic changes to the ranks. The U.S. is now No. 1, with its fast and expansive vaccine rollout, dominated by the highly effective Messenger RNA shots, stemming what was once the world’s worst outbreak.
declined to hear an appeal of a lower court decision upholding the Department of Health and Human Services’ (HHS’) site-neutral payments policy.
The appeal was requested by the American Hospital Association (AHA) in February as part of a multiyear legal battle challenging HHS’ authority to bring Medicare payments to off-campus clinics in line with independent physician practices. The AHA’s bid was supported by a long list of other provider industry stakeholders.
By taking a pass on the case, the top court has now paved the way for HHS to move forward with the 2019 Outpatient Prospective Payment System rule—a policy the agency has said would have saved the Centers for Medicare & Medicaid Services roughly $800 million in payments to outpatient departments during 2020. * * *
HHS’ rule aims to remove payment disparities where hospital-affiliated clinics receive more Medicare reimbursement than physicians’ offices providing the same services. Researchers have suggested over the years that these disparities have played a part in provider consolidation.
Also today the Department of Health and Human Services released a third notice of Affordable Care Act Benefit and Payment Parameters as a proposed rule. Fierce Healthcare informs us that the proposed rule would set the ACA’s open season at an expanded November 1 through January 15 and also would allow exchanges to offer special enrollment periods for low income customers who may benefit from the American Rescue Plan’s expanded premium credits. Health Payer Intelligence discusses two impacts from the current ongoing special ACA open enrollment period which runs until August 15.
In other round up items
The ICD-10 Monitor tells us that the Centers for Disease Control released new ICD-10-CM codes for federal fiscal year 2022 which include 19 new social determinants of health codes in the “Z” chapter. Many of these new “Z” codes are attributable to the Gravity Project which is an HL7 FHIR accelerator organization.
The Wall Street Journal discusses what doctors want their patients to know about the new Alzheimer’s disease drug Aduhelm. For example, “The treatment would work over years, not weeks or months. Dr. [Paul] Aisen estimates that patients with mild cognitive impairment, which is often a precursor to dementia, might get an extra year or two before they start losing their ability to function independently.”
Future demand for healthcare services will be relatively flat to declining, with little to no effect from the COVID-19 pandemic, according to a new forecast report.
At the same time, hospitals and health systems are facing increasing competition from consumer businesses such as Amazon and Walmart, retail behemoths that are rapidly expanding the supply of healthcare services.
The implications of softening demand and increasing supply suggest that pricing trends are ultimately unsustainable for healthcare providers, according to a new report from health system analytics company Trilliant Health.
The company’s analysis, based on 70 billion medical claims across 309 million patient visits, contradicts the commonly held belief that the demand for healthcare services nationwide is rising, according to Sanjula Jain, Ph.D., senior vice president of market strategy and chief research officer at Trilliant Health.
OPM Headquarters a/k/a the Theodore Roosevelt Building
OPM’s new Director Kiran Ahuja was sworn in today. Here is a link to the OPM press release on the festivities.
Health Payer Intelligence informs us that “The Alliance of Community Health Plans (ACHP) has proposed a number of recommendations to improve the Federal Employees Health Benefits (FEHB) program’s plan comparison tool in order to boost quality and enrollment, according to a recent issue brief.” ACHP’s action is timely because OPM has been focusing attention on the plan comparison tool in consultation with interested carriers and presumably other stakeholders.
According to a Committee press release, “The House Appropriations Subcommittee on Financial Services and General Government today approved by voice vote its fiscal year 2022 bill. [This is the bill that funds OPM and the FEHB.] For fiscal year 2022, the draft bill includes $29.1 billion in funding, an increase of $4.8 billion over 2021.”
Sen. Chuck Grassley (R-Iowa) today joined Senate Majority Whip Dick Durbin (D-Ill.) Sen. Angus King (I-Maine) to introduce the Drug-price Transparency for Competition (DTC) Act, a bill that would require price disclosures on advertisements for prescription drugs, in order to empower patients and reduce spending on medications. Last week, the Government Accountability Office (GAO) released a report – requested by Durbin and Grassley – which found direct-to-consumer (DTC) advertisements of prescription drugs contribute to an enormous amount of Medicare costs. Specifically, the DTC Act would require DTC advertisements for prescription drugs and biological products to include a disclosure of the list price, so that patients can make informed choices when inundated with drug commercials.
Speaking of drug prices, let’s take a look at recent news on the new Alzheimer’s Disease drug, Aduhelm.
Yesterday, Biogen issued a bulleted defense of its pricing, which is $56,000 annually per patient. STAT News points out “For families and physicians grappling with the historic approval this month of the controversial Alzheimer’s drug Aduhelm, there’s no shortage of unanswered questions. But a critical one has largely been overlooked: Once patients start taking the medication, how will they know when it’s time to stop? “We don’t have any guidance on how long to give this medication to someone who doesn’t experience adverse events,” said William Mantyh, a behavioral neurologist at M Health Fairview University of Minnesota Medical Center. “With a drug like aducanumab where the upfront demonstrated efficacy is up in the air, it really makes it hard for a clinician to figure out when to stop the drug based on a patient’s clinical symptoms.”
Axios interviewed AHIP CEO Matt Eyles on Aduhelm pricing. In response to an Axios question on acceptable pricing, Mr. Eyles responded that “The best information we have is what [the Institute for Clinical and Economic Review] puts out.” ICER stated on June 7 that “At the ICER public meeting on aducanumab on July 15, 2021, we will tackle important questions [about Aduhem] with all stakeholders at the table. We will also address the question of fair pricing for a drug that now seems likely to become one of the top selling drugs in the history of the United States. ICER’s preliminary draft report calculated a fair annual price to lie between $2,500-$8,300. Even in our most optimistic cost-effectiveness scenario — which ignores the contradictions within the two pivotal trials and presumes that only the positive trial captures the true benefits of treatment — aducanumab’s health gains would support an annual price between $11,100-$23,100. The list price of $56,000 per year announced today by the drug maker far exceeds even this optimistic scenario. Our report notes that only a hypothetical drug that halts dementia entirely would merit this pricing level. The evidence on aducanumab suggests that, at best, the drug is not nearly this effective. Nonetheless, even at the lower range of the estimated number of eligible patients, at this price the drug maker would stand to receive well in excess of $50 billion per year even while waiting for evidence to confirm that patients receive actual benefits from treatment.
The Wall Street Journal reports that “Eli Lilly & Co. plans to submit its Alzheimer’s drug for market clearance under an expedited review this year, in a sign that regulators are encouraging development of treatments for the disease after a recent approval. Lilly said Thursday that the U.S. Food and Drug Administration had designated the company’s experimental Alzheimer’s drug, called donanemab, for the agency’s accelerated approval process. The FDA decision comes after the agency cleared Biogen Inc.’s Aduhelm, the first Alzheimer’s therapy to receive approval in nearly two decades but one that has drawn criticism from doctors and researchers skeptical the drug works. * * * Donanemab performed better in a trial than Biogen’s drug did in its trials, and health insurers and patients would probably prefer it over Aduhelm, J.P. Morgan analyst Chris Schott said in a note to investors.“Donanemab’s approval would be a major blow to Aduhelm’s commercial prospects,” Brian Skorney, a Robert W. Baird & Co. analyst, said in a research note. “We think it would make zero sense for FDA to approve Aduhelm, but not donanemab.” Ah, competition.
In other drug pricing news, Fierce Healthcare tells us that
Cigna is launching a new program that aims to incentivize eligible members to switch to biosimilar drugs.
Under the new Shared Savings Program, members will be offered a one-time $500 debit card for healthcare services or medications if they make the decision to switch to a biosimilar, according to an announcement provided first to Fierce Healthcare.
The program will be made available first to [approximately 7,000] eligible patients taking Remicade, a brand-name biologic that treats a number of inflammatory conditions such as Crohn’s disease and psoriasis. Remicade infusion costs can vary, but Cigna claims data suggest the average regimen costs $30,000 per year, with expenses growing depending on the site of administration.
Two biosimilars for the drug, Avsola and Inflectra, will be moved to the insurer’s preferred tier in July. Eligible customers and their providers will be notified by Cigna about their eligibility to participate in the Shared Savings Program in the coming weeks, the insurer said.
In COVID-19 news —
Fierce Biotech reports that “The FDA green-lit its first antibody test that doesn’t use blood samples to check for evidence of a COVID-19 infection and instead relies on simple, painless mouth swabs. Developed by Diabetomics, the rapid, lateral-flow diagnostic received an agency emergency authorization allowing it to be used at the point of care for adults and children. Designed to deliver a result within 15 minutes, the CovAb test also does not require any additional hardware or instruments. When administered at least 15 days after the onset of symptoms, when the body’s antibody response reaches higher levels, the test demonstrated a false-negative rate of less than 3% and a false-positive rate of nearly 1%, according to the company.”
The New York Times reports that the Baltimore Maryland factory that had been producing the single dose Johnson & Johnson COVID-19 vaccine remains shuttered which Congress investigates its owner Emergent Biosolutions.
The NIH Director’s blog informs us about new NIH research on how Immunity generated from COVID-19 vaccines differs from an Infection. “The good news so far is that, unlike the situation for the common cold, we have now developed multiple COVID-19 vaccines. The evidence continues to suggest that acquired immunity from vaccines still offers substantial protection against the new variants now circulating around the globe. The hope is that acquired immunity from the vaccines will indeed produce long-lasting protection against SARS-CoV-2 and bring an end to the pandemic. These new findings point encouragingly in that direction. They also serve as an important reminder to roll up your sleeve for the vaccine if you haven’t already done so, whether or not you’ve had COVID-19. Our best hope of winning this contest with the virus is to get as many people immunized now as possible. That will save lives, and reduce the likelihood of even more variants appearing that might evade protection from the current vaccines.” Amen to that.
In a bit of Thursday miscellany
Patient Engagement reports that “Optum is bringing healthcare right into Utah’s backyard, rolling out a new Optum Mobile Health Clinic to improve care access for individuals in Optum Care Network Utah. The mobile health clinic, a 45-foot-long vehicle with two private exam rooms, a waiting room, and an imaging lab, is set to address the leading care access barriers experienced by Utahns.” Well done.
A friend of the FEHBlog called his attention to the NIH report on an engaging study suggesting scientists may need to rethink which genes control aging.
We use cookies on our website to give you the most relevant experience by remembering your preferences and repeat visits. By clicking “Accept”, you consent to the use of ALL the cookies.
This website uses cookies to improve your experience while you navigate through the website. Out of these, the cookies that are categorized as necessary are stored on your browser as they are essential for the working of basic functionalities of the website. We also use third-party cookies that help us analyze and understand how you use this website. These cookies will be stored in your browser only with your consent. You also have the option to opt-out of these cookies. But opting out of some of these cookies may affect your browsing experience.
Necessary cookies are absolutely essential for the website to function properly. These cookies ensure basic functionalities and security features of the website, anonymously.
Cookie
Duration
Description
cookielawinfo-checbox-analytics
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Analytics".
cookielawinfo-checbox-functional
11 months
The cookie is set by GDPR cookie consent to record the user consent for the cookies in the category "Functional".
cookielawinfo-checbox-others
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Other.
cookielawinfo-checkbox-necessary
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookies is used to store the user consent for the cookies in the category "Necessary".
cookielawinfo-checkbox-performance
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Performance".
viewed_cookie_policy
11 months
The cookie is set by the GDPR Cookie Consent plugin and is used to store whether or not user has consented to the use of cookies. It does not store any personal data.
Functional cookies help to perform certain functionalities like sharing the content of the website on social media platforms, collect feedbacks, and other third-party features.
Performance cookies are used to understand and analyze the key performance indexes of the website which helps in delivering a better user experience for the visitors.
Analytical cookies are used to understand how visitors interact with the website. These cookies help provide information on metrics the number of visitors, bounce rate, traffic source, etc.
Advertisement cookies are used to provide visitors with relevant ads and marketing campaigns. These cookies track visitors across websites and collect information to provide customized ads.