Both Houses of Congress will be in session this week for Committee business and floor voting. It should be noted that for the next several weeks that FEHBlog will be writing from Austin, TX, way outside the Capital Beltway.
On the COVID-19 front
The American Medical Association offers an article on what doctors would like their patients to know about COVID-19 variants.
The Wall Street Journal reports on the efforts of Pfizer, Merck and the Japanese drugmaker Shionogi to develop a pill to treat COVID-19. “Drugmakers are looking for a pill that those who get a positive Covid-19 test could take at home while their symptoms are mild. Such medicines already exist for influenza, including Roche Holding AG’s Tamiflu and Shionogi’s Xofluza, although they don’t work for all patients and might be prescribed too late to do much good. Xofluza is marketed in the U.S. by Roche. ‘Our target is a very safe oral compound, like Tamiflu, like Xofluza,’ said Isao Teshirogi, Shionogi’s chief executive officer. He said Shionogi’s Covid-19 pill aims to neutralize the virus five days after a patient takes it.” In contrast to the convenience of pills, existing COVID-19 treatments must be administered by a doctor in a hospital or other healthcare facility.
On the regulatory front
The American Hospital Association provides more background on the last week’s proposed Calendar Year 2022 Medicare Part B payment rule. The public comment deadline is September 17.
Kaiser Health News reports on Biogen’s rather aggressive response to criticism of its FDA approval Alzheimer’s Disease drug Aduhelm which was rolled out last week.
In other news —
AHIP discusses health insurer efforts to address provider burnout stemming from the pandemic.
Fierce Healthcare reports that UnitedHealthcare, the largest insurer in the country, will make Peloton’s fitness classes to nearly 4 million fully insured members at no cost through its app, beginning on Sept. 1, the company announced. Eligible members will have access to either a 12-month Peloton digital subscription or a four-month waiver for a Peloton All-Access Membership, the insurer said. All-Access members can take fitness classes through connected devices, such as Peloton’s bikes, and track their metrics, in addition to app access.”
Fierce Healthcare also informs us that “Anthem and Humana have signed on for a minority stake in a new joint venture that aims to reshape the claims management experience. DomaniRx, pending regulatory approval, will feature a cloud-native, API-driven claims adjudication platform, according to an announcement. SS&C Technologies, which provides services and software to the financial and healthcare industries, will have a majority stake in the venture. * * * The goal of the venture, according to the announcement, is to arm healthcare organizations with “end-to-end transparency and data analytics” to help them keep up with an ever-changing regulatory environment.”
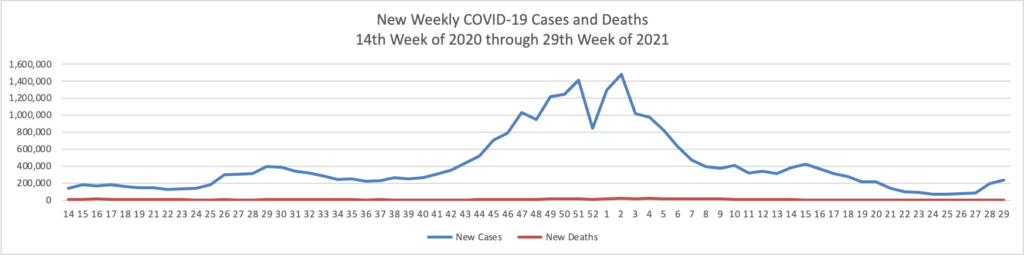
Based on the Centers for Disease Control’s COVID-19 Data Tracker website, here is the FEHBlog’s chart of new weekly COVID-19 cases and deaths over the 14th week of 2020 through 29th week of this year (beginning April 2, 2020, and ending July 21, 2021; using Thursday as the first day of the week in order to facilitate this weekly update):
and here is the CDC’s latest overall weekly hospitalization rate chart for COVID-19:
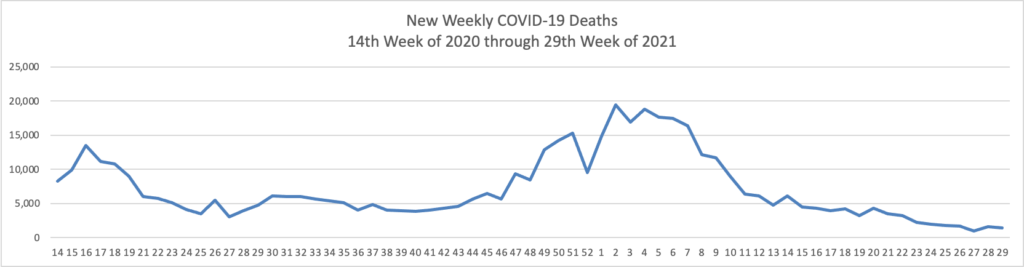
The FEHBlog has noticed that the new cases and deaths chart shows a flat line for new weekly deaths because new cases materially exceed new deaths. Accordingly here is a chart of new COVID-19 deaths over the period (April 2, 2020, through July 21, 2021):
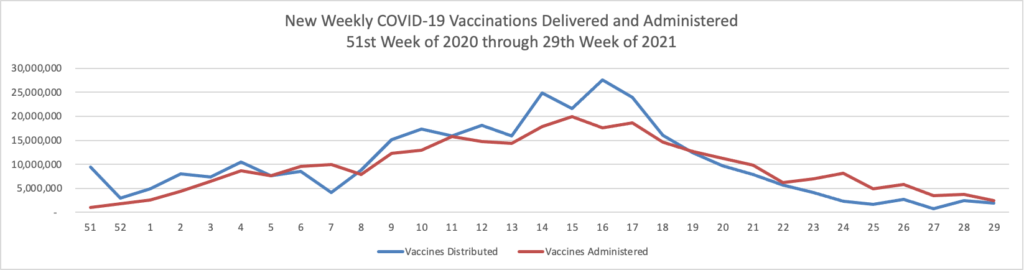
Finally here is a COVID-19 vaccinations chart over the period December 17, 2020, through July 21, 2021, which also uses Thursday as the first day of the week:
Fortune has an excellent, chart-filled article about where we stand with COVID-19. According to the CDC, as of today, nearly half of the total U.S. population (48.9%) is fully vaccinated.
The New York Times reports that “As Israel struggles with a new surge of coronavirus cases, its health ministry reported on Thursday that although effectiveness of the Pfizer-BioNTech vaccine remains high against severe illness, its protection against infection by the coronavirus may have diminished significantly compared with this winter and early spring.” Of course, Pfizer and Moderna have developed a third booster shot, and the Times adds that “Senior [Biden Administration] officials now say they expect that people who are 65 and older or who have compromised immune systems will most likely need a third shot from Pfizer-BioNTech or Moderna, two vaccines based on the same technology that have been used to inoculate the vast majority of Americans thus far. That is a sharp shift from just a few weeks ago, when the administration said it thought there was not enough evidence to back boosters yet.”
STAT News asks and answers burning questions about the COVID-19 pandemic and here is the conclusion
Does Delta mean we’re not going to eradicate Covid-19?
Covid-19 isn’t going to be eradicated, but that was the reality before Delta came around.STAT+:
Remember, the long game with the virus is that our bodies become so used to recognizing it and warding it off that, over time, it becomes little more than a nuisance. With each exposure to the virus, either through an infection or an exposure-mimicking vaccine, our bodies get retrained to fight it. Eventually, SARS-CoV-2 is likely to join the ranks of respiratory viruses that cause occasional colds, with rare exceptions of serious illness.
A reasonable goal indeed.
Becker’s Hospital Review interviews AHIP’s President Matt Eyles. Here’s a snippet:
Q: What do you think are the top three biggest challenges facing payers at this time?
ME: I’d say continuing to navigate the COVID and post-COVID environment, what the impact is going to be with respect to patients who have deferred care as a result of the pandemic — what will the new normal look like?
I think another area is how do we make sure that we have lasting impacts from the shift to telehealth, and that we continue to move forward with respect to making sure that that becomes a really important part of the permanent landscape post-COVID, but that also is designed in a way so that it doesn’t just become another cost increase because more people are just accessing it through different channels and we’re not actually acting more efficiently.
So I’d say those are probably two of the bigger challenges. And then I think third is how we continue to evolve the system toward a more value-based system and an interoperable one that ensures patients have access to the consumer tools and prices they need to make informed healthcare decisions. It’s an incredibly complex effort. It’s one that we absolutely need to move forward with in the right way. But I think some of the timetables that we’re looking for with respect to implementation are very challenging right now in terms of getting to a truly interoperable healthcare system that shares information seamlessly between providers, payers and consumers.
Finally, Deloitte Consulting opines that health and wellness have become CEO priorities in an detail insight publication.
Fierce Healthcare tells us that “Johnson & Johnson’s COVID-19 vaccine presents greater benefits than it does safety risks, especially amid the quickly spreading Delta variant, a key CDC expert panel [,the Advisory Committee on Immunization Practices] decided [today]. However, the panel said that a ruling over the need for a booster added to all COVID shots will have to start with the FDA.”
Fedweek reports that “Federal employees, their unions and members of Congress continue to watch for details of federal agency ‘reentry’ and ‘post-reentry’ operational plans, with the deadline having passed on Monday (July 19) for agencies to submit those plans to OMB but with changes to telework and other workplace policies likely still weeks or months away.”
Senators Patrick Leahy (D-Vt.) and Steve Daines (R-Mont.) on Tuesday [July 20] requested updates from both the Federal Trade Commission (FTC) and the Department of Justice (DOJ) on their recent efforts to combat anticompetitive conduct in the health insurance industry. The two senators recently served as chief cosponsors of the bipartisan Competitive Health Insurance Reform Act (CHIRA), which protects consumers by repealing a long-outdated antitrust exemption for the health insurance industry. Decades of consolidation by health insurance brokers has primed the industry for abuse, allowing insurers to exert market power in order to raise premiums, restrict competition, and deny consumers choice.
Since the CHIRA’s passage in January of this year, neither the FTC nor the DOJ has announced major steps to exercise their expanded antitrust enforcement authority under the new law. In their letter, the senators called on the agencies to provide information on any enforcement actions, guidelines, rulemaking, or other actions taken to extend antitrust enforcement to the health insurance industry since then.
Following up on Mondays’ ACA FAQ 47, HHS today announced “the launch of The HIV Challenge, a national competition to engage communities to reduce HIV-related stigma and increase prevention and treatment among racial and ethnic minority people. Through this challenge, HHS is seeking innovative and effective approaches to increase the use of pre-exposure prophylaxis medication (PrEP) and antiretroviral therapy (ART) among people who are at increased risk for HIV or are people with HIV. The HIV Challenge is open to the public, and HHS will award a total of $760,000 to 15 winners over three phases. Phase 1 submissions are open from July 26, 2021, through September 23, 2021.”
Kaiser Health News explains how the Centers for Medicare and Medicaid Services is reevaluating its wellness program for pre-diabetic Medicare beneficiaries.
Over the past decade, tens of thousands of American adults of all ages have taken these diabetes prevention classes with personalized coaching at YMCAs, hospitals, community health centers and other sites. But out of an estimated 16 million Medicare beneficiaries whose excess weight and risky A1c level make them eligible, only 3,600 have participated since Medicare began covering the two-year Medicare Diabetes Prevention Program (MDPP) in 2018, according to the federal government’s Centers for Medicare & Medicaid Services (CMS).
Researchers and people who run diabetes prevention efforts said participation is low because of the way Medicare has set up the program. It pays program providers too little: a maximum of $704 per participant, and usually much less, for dozens of classes over two years. It also imposes cumbersome billing rules, doesn’t adequately publicize the programs and requires in-person classes with no online options, except during the pandemic emergency period. Most of the private Medicare Advantage plans haven’t promoted the program to their members.
Now, CMS has proposed to address some but not all of those problems in a rule change. It predicted the changes would reduce the incidence of diabetes in the Medicare population and potentially cut federal spending to treat diabetes-related conditions.
Leveraging Food and Drug Administration regulations loosened during the pandemic, Happify Health, which is best known for its consumer wellness app, will launch new prescription-only software to treat depression.
Happify, founded in 2012, recently announced it had raised $73 million to bolster its efforts in digital therapeutics, a space that is rapidly growing as well-funded companies make the case to regulators, insurers, and clinicians that software can be used to treat disease.
The new product, called Ensemble, is designed to treat both major depressive disorder and generalized anxiety disorder. The software, accessible on both computers and smartphones, guides patients through 10 weeks of cognitive behavioral therapy, or CBT, and other related techniques aimed at changing behavior patterns and teaching coping skills.
The FEHBlog likes the company’s name.
The American Medical Association wants the Food and Drug Administration to loosen up on its opioid prescribing rules which conflict with patient care. Perhaps the FEHBlog is oversimplifying this issue, but haven’t we been down this road to perdition before?
Large tech giants are jumping into a growing interoperability solutions market as new federal regulations spur the healthcare industry to open up and share medical records data.
Google Cloud rolled out a new tool called the healthcare data engine, currently in private preview, that helps healthcare and life sciences organizations harmonize data from multiple sources, including medical records, claims, clinical trials and research data.
It gives organizations a holistic view of patient longitudinal records, and enables advanced analytics and AI in a secure and compliant cloud environment, according to Google Cloud executives.
Yesterday, “at her first meeting of the Chief Human Capital Officers (CHCO) Council, Office of Personnel Management (OPM) Director and Council Chair, Kiran Ahuja, announced that the CHCO Council’s functions will be restored to OPM, after the Council’s leadership and administration were bifurcated between OPM and General Services Administration (GSA) since 2019.” Sic semper attempted GSA merger.
The North Carolina Attorney General announced “a historic $26 billion agreement that will help bring desperately needed relief to people across the country who are struggling with opioid addiction. The agreement includes Cardinal, McKesson, and AmerisourceBergen – the nation’s three major pharmaceutical distributors – and Johnson & Johnson, which manufactured and marketed opioids. The agreement also requires significant industry changes that will help prevent this type of crisis from ever happening again. The agreement would resolve investigations and litigation over the companies’ roles in creating and fueling the opioid epidemic. State negotiations were led by Attorneys General Josh Stein (NC) and Herbert Slatery (TN) and the attorneys general from California, Colorado, Connecticut, Delaware, Florida, Georgia, Louisiana, Massachusetts, New York, Ohio, Pennsylvania, and Texas.”
Healthcare Dive informs us that “Anthem, the nation’s second largest insurer [and a Blue Cross licensee], saw robust membership growth during the second quarter, adding 1.9 million members, a 4.4% increase over the prior-year period. The growth was fueled entirely by government programs, largely Medicaid and Medicare, while commercial membership declined slightly. The Indianapolis-based insurer raised its forecast for the full year as its performance in the second quarter outperformed expectations. Even though COVID-19 cases continue to rise due to the delta variant and non-COVID-19 care resumes, Anthem’s medical loss ratio of 86.8% came in below company and analyst expectations.”
Healthcare Dive further reports that “Americans’ medical debtmay have reached $140 billion last year, significantly higher than past estimates and outweighing all other types of personal debt in the U.S., according to a new study published in JAMA. Researchers analyzed a tenth of all credit reports from rating agency TransUnion to find nearly one in five Americans had medical debt in collections in June last year — more than any other type. Debt was significantly more concentrated in states that had yet to expand Medicaid under the Affordable Care Act. The analysis reflects care provided prior to COVID-19, but early data shows the pandemic has likely only exacerbated the perennial issue of medical debt in the U.S.” The FEHBlog is surprised that one decade into the Affordable Care Act this issue has not diminished.
In another downbeat but important story, AHIP tells us that “price gouging on COVID-19 tests by certain providers continues to be a widespread problem, threatening patients’ ability to get the testing they need.”
The FEHBlog also ran across the following three interesting articles in Forbes:
“Most hospital executives will say it’s impossible to run a business on Medicare rates. The government health insurance program for seniors pays less for services than it costs to deliver them and private insurance has to make up the difference. But Eren Bali doesn’t buy the cost-shifting argument. The serial entrepreneur who grew up in rural southeast Turkey believes the issue isn’t the rates but an outdated system using old technology. “There’s so much waste because providers are so used to charging through the roof in this country, they’ve never thought about being efficient,” says Bali, 37, the CEO and cofounder of Carbon Health.” This article is a day brightener.
“UnitedHealth Group is rolling out an increasing number of partnerships to “address health equity challenges” across the U.S.” The article adds that “UnitedHealth’s effort comes as the company and rivals including Anthem, CVS Health’s Aetna health plan unit, Humana and others address social determinants of health as insurers intensify strategies to reduce costs and improve outcomes beyond covering traditional medical treatments.”
“The coronavirus pandemic forced many hospitals to confront an uncomfortable truth: they were sitting on troves of patient data but, despite tens of millions of dollars spent on electronic health records and IT infrastructure, couldn’t extract useful insights to help treat the virus ravaging the wards. This experience was the tipping point that pushed a group of 17 hospitals to come together, including three new members announced this week, to raise $95 million for a startup called Truveta.” The article adds that “The aim of the company is to enable hospitals to monetize patient data that has been de-identified in ways that may both improve existing treatments and develop new ones. With the addition of Texas-based Baylor Scott & White Health, Maryland-based MedStar Health and Texas Health Resources, the hospital-governed Truveta now says it represents organizations that provide 15% of patient care in the United States. The Seattle, Washington-based startup is helmed not by a veteran of the healthcare world, but by former Microsoft executive Terry Myerson, who’s better known for his work on Windows and Xbox.”
David Leonhardt in the New York Times offered an encouraging article this morning:
When the Kaiser Family Foundation conducted a poll at the start of the year and asked American adults whether they planned to get vaccinated, 23 percent said no.
But a significant portion of that group — about one quarter of it — has since decided to receive a shot. The Kaiser pollsters recently followed up and asked these converts what led them to change their minds. The answers are important, because they offer insight into how the millions of still unvaccinated Americans might be persuaded to get shots, too.
What helps move people from vaccine skeptical to vaccinated? The Kaiser polls point to three main themes.
(The themes apply to both the 23 percent of people who said they would not get a shot, as well as to the 28 percent who described their attitude in January as “wait and see.” About half of the “wait and see” group has since gotten a shot.)
1. Seeing that millions of other Americans have been safely vaccinated. * * *
2. Hearing pro-vaccine messages from doctors, friends and relatives. * * * and
3. Learning that not being vaccinated will prevent people from doing some things.
That’s helpful information for the many vaccine advocates, among us.
Today was a busy day for regulatory action:
The Secretary of Health and Human Services renewed for another 90 day period the COVID-19 public health emergency. Earlier this month, the HHS Secretary issued a similar renewal for the Opioid public health emergency which of course predates the COVID-19 emergency. Here’s a link discussing the actions that the federal government can take in response to a public health emergency declaration.
The Affordable Care Act regulators issued implementation guidance FAQs part 47 today. As background, “on June 11, 2019, the U.S. Preventive Services Task Force released a recommendation with an “A” rating that clinicians offer [pre-exposure prophylaxis (PrEP)] with “effective antiretroviral therapy to persons who are at high risk of human immunodeficiency virus (HIV) acquisition.” Accordingly, [as required by the ACA, non-grandfathered] plans and issuers must cover PrEP consistent with the USPSTF recommendation without cost sharing [when provided in-network] for plan years (in the individual market, policy years) beginning on or after one year from the issue date of the recommendation (in this case, plan or policy years beginning on or after June 30, 2020).” The FAQs concern the scope of the requisite no cost sharing coverage for this particular service. Affected plans and issuers are allowed sixty days to implement the guidance.
The Centers for Medicare and Medicaid Services “proposed Medicare payment rates for hospital outpatient and Ambulatory Surgical Center (ASC) services. The Calendar Year (CY) 2022 Hospital Outpatient Prospective Payment System (OPPS) and ASC Payment System Proposed Rule is published annually and will have a 60-day comment period, which will end on September 17, 2021.” Here is a link to the fact sheet on the proposal. Consistent with the President’s recent executive order on competition, the CMS rule making “proposes to set a minimum CMP of $300/day that would apply to smaller hospitals with a bed count of 30 or fewer and apply a penalty of $10/bed/day for hospitals with a bed count greater than 30, not to exceed a maximum daily dollar amount of $5,500. Under this proposed approach, for a full calendar year of noncompliance, the minimum total penalty amount would be $109,500 per hospital, and the maximum total penalty amount would be $2,007,500 per hospital.” That should be attention getting if finalized. Also the rule making proposes to backtrack on Trump Administration CMS rules that would phase out inpatient only Medicare requirements for certain medical procedures. The former administration’s goal was to lower costs, but the current administration finds that the former administration did not follow all of the necessary patient safety procedural requirements when making this change.
Govexec reports that today “marks the deadline for agencies to submit their finalized return to office plans to the Office of Management and Budget. These plans, which are not intended to be public, will vary by agency.”
The American Hospital Association informs us that “The Centers for Medicare & Medicaid Services will host a national stakeholders call July 22 at 3:30 p.m. ET on the interim final rule, Surprise Billing Part 1, that implements aspects of the No Surprises Act that bans balance billing in certain out-of-network scenarios. The call-in number is 888-455-1397; the participant passcode is 8758359.” Thanks AHA and CMS.
Both Houses of Congress are in session this week for Committee business and floor voting. Roll Call reports that the House of Representatives is expected to hold a floor vote on a minibus appropriations bill including OPM appropriations during the week of July 26.
On the COVID-19 front —
Fierce Healthcare reports that “This is becoming a pandemic of the unvaccinated,” said Rochelle Walensky, M.D., director of the Centers for Disease Control and Prevention, during a briefing Friday [July 16]. “We are seeing outbreaks of cases in parts of the country that have low vaccination coverage because unvaccinated people are at risk. Communities that are fully vaccinated are generally faring well.” On the brighter side, “States with the highest cases are starting to see their vaccination rates go up, [Jeff] Zients {the White House coronavirus response coordinator] said [at the same briefing]. ‘In the past week, the five states with the highest case rates had a higher rate of people getting newly vaccinated compared to the national average,’ he added.”
In Friday’s post the FEHBlog noted that the Food and Drug Administration has fast tracked the Pfizer – Biotech application for full FDA approval of its COVID-19 vaccine. Precision Vaccinations tells us that “The Prescription Drug User Fee Act goal date for a decision by the U.S. FDA is in January 2022.”
Looking ahead, the JAMA Network offers an interesting article on the search for a single vaccine against coronaviruses yet to come.
On the telehealth front, Becker’s Hospital Review discusses how Amazon, Walmart and seven others have been expanding their respective telehealth businesses in 2021.
On the fraud waste and abuse front, Kaiser Health News reports that
Tens of thousands of times a year, hospitals charge enormously expensive trauma alert fees for injuries so minor the patient is never admitted.
In Florida alone, where the number of trauma centers has exploded, hospitals charged such fees more than 13,000 times in 2019 even though the patient went home the same day, according to a KHN analysis of state data provided by Etienne Pracht, an economist at the University of South Florida. Those cases accounted for more than a quarter of all the state’s trauma team activations that year and were more than double the number of similar cases in 2014, according to an all-payer database of hospital claims kept by Florida’s Agency for Health Care Administration.
While false alarms are to be expected, such frequent charges for little if any treatment suggest some hospitals see the alerts as much as a money spigot as a clinical emergency tool, claims consultants say.
“Some hospitals are using it as a revenue generator,” Tami Rockholt, a registered nurse and medical claims consultant who appeared as an expert witness in the Sutter Health car-accident trial, said in an interview. “It’s being taken advantage of” and such cases are “way more numerous” than a few years ago, she said.
Finally, the American Medical Association offers common sense views on what doctors wish their patients knew about healthy eating.
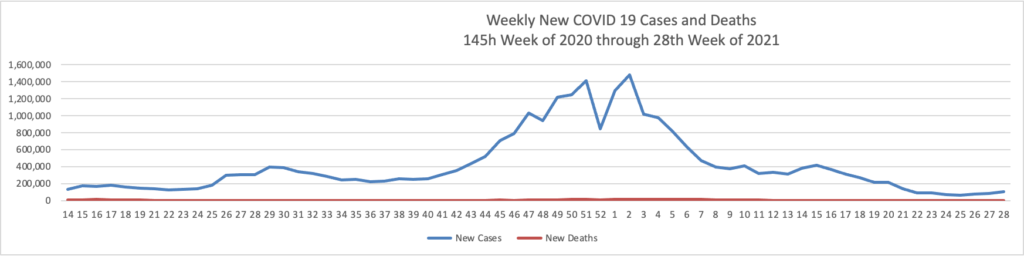
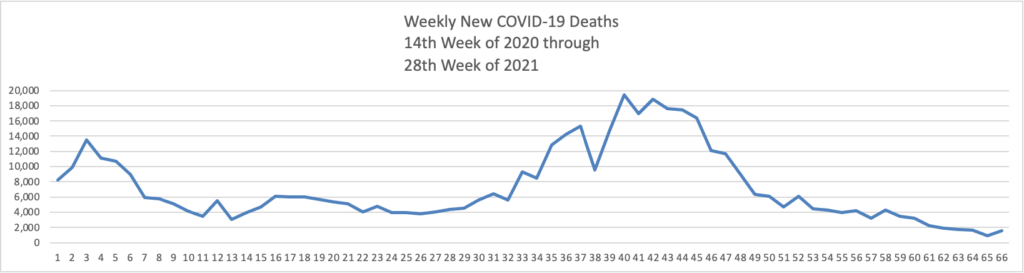
Based on the Centers for Disease Control’s COVID-19 Data Tracker website, here is the FEHBlog’s chart of new weekly COVID-19 cases and deaths over the 14th week of 2020 through 28th week of this year (beginning April 2, 2020, and ending July 14, 2021; using Thursday as the first day of the week in order to facilitate this weekly update):
and here is the CDC’s latest overall weekly hospitalization rate chart for COVID-19:
The FEHBlog has noticed that the new cases and deaths chart shows a flat line for new weekly deaths because new cases materially exceed new deaths. Accordingly here is a chart of new COVID-19 deaths over the period (April 2, 2020, through July 14, 2021):
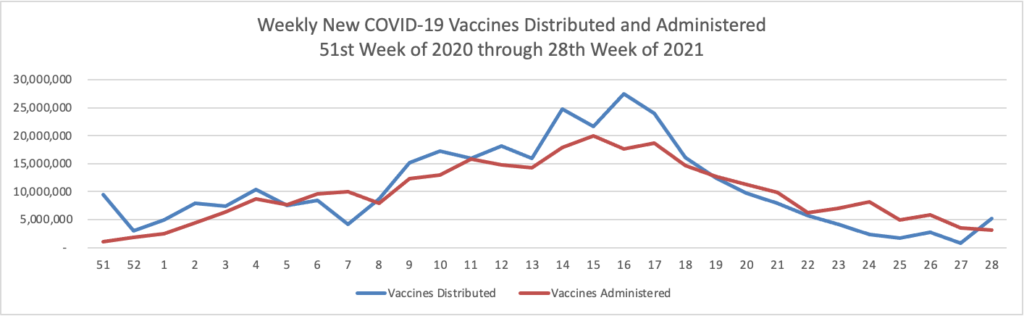
Finally here is a COVID-19 vaccinations chart over the period December 17, 2020, through July 14, 2021 which also uses Thursday as the first day of the week:
As of today, according to the Centers for Disease Control, 160.7 million Americans are fully vaccinated against COVID-19, which figure represents 59.6% of the population eligible to be vaccinated (age 12 and up). 79.3% of the population over age 65 is fully vaccinated. That’s a key fact.
The American Hospital Association informs us that “Pfizer today said its COVID-19 vaccine will receive a priority review from the Food and Drug Administration, indicating that Pfizer has completed its rolling submission of its application for the vaccine’s full authorization. The company’s Biologics License Application, which is intended for individuals age 16 and older, is supported by clinical date from its phase 3 clinical trial.” That’s good news.
The Washington Post reports that “A federal advisory panel [the CDC’s Advisory Committee on Immunization Practices] is expected next week to consider whether health-care workers should be allowed to give additional coronavirus shots to patients with fragile immune systems, even as top U.S. health officials have said an additional dose of vaccine is not widely needed. * * * The advisory panel[on July 22] plans to focus on the 2 to 4 percent of U.S. adults who have suppressed immunity, a population that includes organ transplant recipients, people on cancer treatments and people living with rheumatologic conditions, HIV and leukemia.”
From the prescription drug front —
STAT News reports that “A prominent panel of medical experts [convened by the Institute of Clinical and Economic Review] unanimously voted that there is no evidence to suggest the recently approved Alzheimer’s drug offers patients any health benefits beyond the usual care. * * * After the voting, a roundtable discussion was held during which Mark McClellan, a former Centers for Medicare & Medicaid Administrator, said that access to Aduhelm “is going to be pretty limited at least until the nine-month period is over” and that we are “not going to see very big numbers in the near term.” This is likely because many payers will want to wait for Medicare to make its coverage decision in early 2022.”
Bloomberg reports that ” When a new obesity medication from the Danish drugmaker Novo Nordisk A/S began selling in the U.S. in June, it became the most effective weight loss drug on the market. Wegovyhelps patients lose an average of about 15% of their body weight, almost double the rates demonstrated by other prescription treatments, according to study results. That translates to a loss of about 20 to 70 pounds for eligible patients. Only costly and invasive bariatric surgery has shown the ability to eliminate more pounds. With more than 100 million people categorized as obese, the U.S. is a potentially huge market for Wegovy, which costs $1,350 for four weekly injections and is being pitched as a long-term therapy. * * * Insurance companies, pharmacy benefit managers, and employers determine whether health plans cover weight loss drugs, and which ones. Today only about half the clients of Cigna Corp.’s Express Scripts unit and Prime Therapeutics LLC, two major pharmacy benefit managers, reimburse for weight loss drugs. Express Scripts recently added Wegovy to its largest formulary, covering about 24 million people. Insurers Anthem Inc. and CVS Health Corp.’s Aetna don’t typically cover weight loss drugs, but both have indicated Wegovy will likely get some coverage. Others have yet to decide. Although “it’s not for everyone,” Wegovy has a role to play in treating obesity, says Amy Bricker, president of Express Scripts. She says she’s optimistic that treating obesity will lower costs for Express Scripts’ health plans.”
HealthTech Magazine offers a useful article on integrating virtual care into a healthcare organization’s overall delivery strategy. During the NCQA / HL7 Digital Quality Measure conference this week more than one doctor remarked that no one has found the Goldilocks level for virtual care, but at least study appears underway.
The FEHBlog realized today that he had neglected to provide this link to Prof. Katie Keith’s comprehensive Health Affairs Blog article on the first No Surprises Act interim final rule. AIS offers the following expert takes on that rule:
Industry experts’ perspectives:
Loren Adler, an associate director at the USC-Brookings Schaeffer Initiative for Health Policy, says that the QPA formula could lock in high rates for providers in some regions, particularly areas where there is a paucity of certain types of providers. He interprets the QPA calculation in the IFR as “a pretty provider-friendly definition. Ge Bai, Ph.D., an associate professor at Johns Hopkins University’s Carey Business School and Bloomberg School of Public Health, says that it’s important to remember the larger picture — the No Surprises Act could reduce physicians’ revenue in some cases. She says that it could exacerbate physician shortages in areas that pay lower rates than others as physicians move to more lucrative locations. Going forward, it’s hard to say whether the law and IFR will have inflationary effects on health care prices overall, Adler says. “The biggest piece of that, the determinant, will be the arbitration process,” he adds. He’s waiting to see what happens when the law actually comes into effect and arbitrations begin to take place.
The FEHBlog hopes that this law will not encourage providers to leave health plan networks.
On the COVID-19 front
David Leonhardt in the New York Times informs us about “Hopeful News on Delta. The Delta variant is more contagious. It does not appear to be more severe.” “If a new variant is not actually more severe, it doesn’t present a greater threat to a typical person who contracts Covid. Vaccinated people would remain protected. For children too young to be vaccinated, serious Covid symptoms would still be exceedingly rare — rarer than many other everyday risks, like riding in a car — and still concentrated among children with other health problems.”
U.S. Surgeon General Dr. Vivek Murthy issued “the first Surgeon General’s Advisory of this Administration to warn the American public about the urgent threat of health misinformation. Health misinformation, including disinformation, have threatened the U.S. response to COVID-19 and continue to prevent Americans from getting vaccinated, prolonging the pandemic and putting lives at risk, and the advisory encourages technology and social media companies to take more responsibility to stop online spread of health misinformation.
On the Aduhelm front:
The Wall Street Journal reports that “A pair of large hospitals are declining to administer Biogen Inc.’s new Alzheimer’s treatment, Aduhelm, the latest rupture to emerge from the Food and Drug Administration’s controversial approval of the drug last month. The Cleveland Clinic and Mount Sinai Health System in New York said they wouldn’t administer Aduhelm, which is also called aducanumab, to patients amid a debate about the drug’s effectiveness and whether the FDA lowered its standards in approving the medicine.”
Healthcare Dive informs us that “On a morning call with investors [today], UnitedHealth leadership said they were waiting on more information before making a coverage decision regarding Aduhelm, Biogen’s expensive new drug for Alzheimer’s disease priced at an average cost of $56,000 per year.”
Normally, if a drug gets FDA approval, that means it has some benefit to patients. But the FDA decided to greenlight Biogen’s controversial drug Aduhelm without that guarantee.
That decision leaves patients, clinicians, and insurance companies in the dark. Under by far the most pressure is Medicare [and FEHB is a close second because FEHB carriers are on the hook for Medicare eligible annuitants drug coverage (see Wednesday’s post)}, since most patients eligible for the pricey drug have insurance through the taxpayer-funded program. Officials with the program just this week started the process for figuring out how Medicare will cover the drug, which will take months.
Some experts and stakeholders, including the influential Alzheimer’s Association, have called on Medicare to activate a rarely used regulatory tool to get more data about how well the drug works. (The FDA has also said Biogen must study whether Aduhelm slows down patients’ cognitive decline, but the drug maker has said it doesn’t have to report its results for another nine years.)
The tool, called a Coverage with Evidence Development, would mean Medicare would only cover Aduhelm for patients who enroll in clinical studies. The process has the potential to create real-world data that could help patients, physicians, and payers navigate unprecedented and difficult decisions.
In miscellaneous news
Healthcare Dive reports that “UnitedHealth Group handily beat Wall Street expectations for earnings and revenue in the second quarter, reporting revenue up 15% year over year to $71.3 billion, leading the Minnesota-based healthcare behemoth to increase its full-year guidance following the results.”
The Department of Health and Human Services announced that “more than two million people have signed up for health coverage during the Biden-Harris Administration’s 2021 Special Enrollment Period (SEP), which opened on February 15, 2021 as the country grappled with the pandemic, and will conclude on the extended deadline August 15, 2021.” * * * “The report also shows that of the new and returning consumers who have selected a plan since April 1, 1.2 million consumers (34%) have selected a plan that costs $10 or less per month after the American Rescue Plan’s (ARP) premium reductions.” The President wants Congress to make permanent this two year long premium reduction program.
Fierce Healthcare adds that “Senate Democrats announced late Tuesday the framework for a $3.5 trillion infrastructure package that will expand Medicare to offer dental, hearing and vision benefits.”
Today, the FEHBlog virtually attended the NCQA Digital Quality Summit. A highlight was a VA healthcare speaker who pointed out the VA’s access to care website which is nifty. The site, for example, includes comprehensive comparisons of VA care versus outside care. The site should be useful to FEHB carriers because the FEHB Program covers a large cadre of veterans.
The Centers for Medicare Services released its proposed calendar year 2022 Medicare Part B physician payment rule. According to the fee schedule fact sheet
With the proposed budget neutrality adjustment to account for changes in RVUs (required by law), and expiration of the 3.75 percent payment increase provided for CY 2021 by the Consolidated Appropriations Act, 2021 (CAA), the proposed CY 2022 PFS conversion factor is $33.58, a decrease of $1.31 from the CY 2021 PFS conversion factor of $34.89. The PFS conversion factor reflects the statutory update of 0.00 percent and the adjustment necessary to account for changes in relative value units and expenditures that would result from our proposed policies.
That would cause a cost shift to commercial carriers.
From the tidbit front —
The first interim final rule implementing the No Surprises Act was published in the Federal Register today. It turns out that the public comment deadline is Tuesday, September 7, 2021.
Many people, including me, have experienced a sense of gratitude and relief after receiving the new COVID-19 mRNA vaccines. But all of us are also wondering how long the vaccines will remain protective against SARS-CoV-2, the coronavirus responsible for COVID-19.
Earlier this year, clinical trials of the Moderna and Pfizer-BioNTech vaccines indicated that both immunizations appeared to protect for at least six months. Now, a study in the journal Nature provides some hopeful news that these mRNA vaccines may be protective even longer [1].
In the new study, researchers monitored key immune cells in the lymph nodes of a group of people who received both doses of the Pfizer-BioNTech mRNA vaccine. The work consistently found hallmarks of a strong, persistent immune response against SARS-CoV-2 that could be protective for years to come.
Though more research is needed, the findings add evidence that people who received mRNA COVID-19 vaccines may not need an additional “booster” shot for quite some time, unless SARS-CoV-2 evolves into new forms, or variants, that can evade this vaccine-induced immunity. That’s why it remains so critical that more Americans get vaccinated not only to protect themselves and their loved ones, but to help stop the virus’s spread in their communities and thereby reduce its ability to mutate.
In other NIH news, NIH researchers report a conundrum:
Medications to treat alcohol use disorder, although effective, are only being used to treat 1.6% of people with the disorder, according to a new study.
The findings show that medications for alcohol use disorder are rarely prescribed, even though approved drugs are available.
In an article that may be helpful for FEHB plans to share with members, the Centers for Disease Control discusses the causes for type 2 diabetes.
Health Payer Intelligence reports that employers are shifting the focus of their wellness programs from physical health to mental health. “Over nine in ten employers said that they were increasing their mental health and wellness programming in 2021, including pediatric mental health programs, according to a survey from Fidelity and Business Group on Health. Almost 75 percent reported that they were extending work-life balance support.and nearly 70 percent were expanding their paid leave policies.”
The New York Times reports that “The Food and Drug Administration warned on Monday that Johnson & Johnson’s coronavirus vaccine can lead to an increased risk of a rare neurological condition known as Guillain–Barré syndrome, another setback for a [one dose] vaccine that has largely been sidelined in the United States. Although regulators have found that the chances of developing the condition are low, they appear to be three to five times higher among recipients of the Johnson & Johnson vaccine than among the general population in the United States, according to people familiar with the decision. The warning was attached to factsheets about the vaccine for providers and patients.”
USA Today offers a success story on AHIP’s Vaccine Community Connectors program. “Most important, this effort helped the industry home in on one specific strategy to accelerate health equity: better access to health care data that incorporates the social determinants of health.” Speaking SDOH data, Health IT Analytics informs us about the use of SDOH data in researching and managing Alzheimer’s Disease.
The American Hospital Association reminded folks today to keep its Vaccine Communications Resources website in mind.
“The Biden administration has started to investigate whether Medicare should cover the extremely pricey Alzheimer’s drug aducanumab. The Centers for Medicare & Medicaid Services announced Monday it is opening a National Coverage Determination (NCD) analysis on the drug that will cost patients $56,000 a year. Advocates and experts have called for the agency to move quickly to decide whether to cover the drug. “We want to consider Medicare coverage of new treatments very carefully in light of the evidence available,” said CMS Administrator Chiquita Brooks-LaSure, in a statement Monday. “That’s why our process will include opportunities to hear from many stakeholders.”
Earlier press reports on Aduhelm, as well as common sense, indicate that commercial health plans likely will follow CMS’s lead on coverage of that drug.
Healthcare Dive tells us that “Telehealth use overall has stabilized at levels 38 times higher than before the COVID-19 pandemic, ranging from 13% to 17% of visits across all specialties, according to new data from McKinsey released roughly a year since the first major spike in COVID-19 cases.” * * * On the provider side, 58% of physicians continue to view virtual care more favorably than before the pandemic, though that’s down slightly from September, when 64% of physicians were in support. As of April this year, 84% of doctors were offering telehealth, and 57% said they’d prefer to continue offering it. However, that’s largely dependent on reimbursement: 54% of doctors said they wouldn’t provide virtual care if it was paid at a 15% discount to physical services.”
HR Dive discusses the President’s July 9 executive order provision “taking aim at” non-compete agreements.
Biden’s order leaves some questions unanswered. It does not ban or impact any existing employment agreement, Chris Marquardt, partner at Alston & Bird, told HR Dive in an email. “Employers will need to wait and see what the Federal Trade Commission does in response to the Executive Order before thinking about its potential impact,” he said.
Among other reasons, intellectual property and trade secrets have been cited as cause for use of non-competes. But the agreements have been the subject of criticism for potentially driving down wages in certain industries and geographic areas.
Govexec.com offers an interesting take on how the July 9 executive order seeks to use Federal procurement and regulations to promote competition
We use cookies on our website to give you the most relevant experience by remembering your preferences and repeat visits. By clicking “Accept”, you consent to the use of ALL the cookies.
This website uses cookies to improve your experience while you navigate through the website. Out of these, the cookies that are categorized as necessary are stored on your browser as they are essential for the working of basic functionalities of the website. We also use third-party cookies that help us analyze and understand how you use this website. These cookies will be stored in your browser only with your consent. You also have the option to opt-out of these cookies. But opting out of some of these cookies may affect your browsing experience.
Necessary cookies are absolutely essential for the website to function properly. These cookies ensure basic functionalities and security features of the website, anonymously.
Cookie
Duration
Description
cookielawinfo-checbox-analytics
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Analytics".
cookielawinfo-checbox-functional
11 months
The cookie is set by GDPR cookie consent to record the user consent for the cookies in the category "Functional".
cookielawinfo-checbox-others
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Other.
cookielawinfo-checkbox-necessary
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookies is used to store the user consent for the cookies in the category "Necessary".
cookielawinfo-checkbox-performance
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Performance".
viewed_cookie_policy
11 months
The cookie is set by the GDPR Cookie Consent plugin and is used to store whether or not user has consented to the use of cookies. It does not store any personal data.
Functional cookies help to perform certain functionalities like sharing the content of the website on social media platforms, collect feedbacks, and other third-party features.
Performance cookies are used to understand and analyze the key performance indexes of the website which helps in delivering a better user experience for the visitors.
Analytical cookies are used to understand how visitors interact with the website. These cookies help provide information on metrics the number of visitors, bounce rate, traffic source, etc.
Advertisement cookies are used to provide visitors with relevant ads and marketing campaigns. These cookies track visitors across websites and collect information to provide customized ads.