Second Interim Final Rule on NSA Implementation Released / Gov’t Shutdown Avoided

Today, the Departments of Health and Human Services, Labor, and Health and Human Services, and OPM issued the second interim final rule on No Surprises Act (“NSA”) implementation. This rule concerns the independent dispute resolution (“IDR”) process. The process is intended to resolve disputes that arise when an out-of-network provider is dissatisfied with the qualifying payment amount (“QPA”) from the health plan pursuant to the NSA.
The IDR process timeline is as follows:
| Independent Dispute Resolution Action | Timeline |
| Initiate 30-business-day open negotiation period | 30 business days, starting on the day of initial payment or notice of denial of payment |
| Initiate independent dispute resolution process following failed open negotiation | 4 business days, starting the business day after the open negotiation period ends |
| Mutual agreement on certified independent dispute resolution entity selection | 3 business days after the independent dispute resolution initiation date |
| Departments select certified independent dispute resolution entity in the case of no conflict-free selection by parties | 6 business days after the independent dispute resolution initiation date |
| Submit payment offers and additional information to certified independent dispute resolution entity | 10 business days after the date of certified independent dispute resolution entity selection |
| Payment determination made | 30 business days after the date of certified independent dispute resolution entity selection |
| Payment submitted to the applicable party | 30 business days after the payment determination |
The NSA IDR process uses the so-called baseball arbitration approach under which the decision maker selects one of the parties proposals rather than craft an independent approach as judges do. The requirements description accompanying the final rule explains
When making a payment determination, certified independent dispute resolution entities must begin with the presumption that the QPA is the appropriate OON amount. If a party submits additional information that is allowed under the statute, then the certified independent dispute resolution entity must consider this information if it is credible. For the independent dispute resolution entity to deviate from the offer closest to the QPA, any information submitted must clearly demonstrate that the value of the item or service is materially different from the QPA. Without this additional information, the certified independent dispute resolution entity must select the offer closest to the QPA.
Basically this instructs the health plan to make a proposal close to, if not equal to, the QPA. Then the burden of proof for a higher amount is necessarily placed on the provider. The FEHBlog’s hunch is supported by the following American Hospital Association (“AHA”) statement from the provider side:
AHA Executive Vice President Stacey Hughes said, “The No Surprises Act was an important step forward in protecting patients from surprise medical bills. Hospitals and health systems strongly support these protections and the balanced approach Congress chose to resolve disputes. Disappointingly, the Administration’s rule has moved away from Congressional intent and brought new life to harmful proposals that Congress deliberately rejected. Today’s rule is a windfall for insurers. The rule unfairly favors insurers to the detriment of hospitals and physicians who actually care for patients. These consumer protections need to be implemented in the right way, and this misses the mark.”
AHA staff are reviewing the rule. Watch for a Special Bulletin tomorrow with additional details.
On the bright side for providers, it appears that the IDR process allows the health plan no opportunity to make a low ball proposal to the decision maker. However, it’s the FEHBlog’s view that the devil remains in the details of this lengthy rule and no one should underestimate the ingenuity of lawyers on either side in these novel legal situations. Finally, the apparently simple approach that the regulators took will facilitate implementing the principal feature of the No Surprises Act on January 1, 2022.
From Capitol Hill, Roll Call reports that
President Joe Biden signed a stopgap funding measure Thursday with hours to spare before federal agencies would otherwise have to start shutting down.
The continuing resolution gives lawmakers and the White House nine more weeks to reach agreement on spending levels and negotiate a dozen fiscal 2022 appropriations bills. * * *
The stopgap bill extends federal agencies’ current spending rates, with some exceptions known as “anomalies,” through Dec. 3, as well as certain expiring program authorizations like the National Flood Insurance Program’s ability to sell new policies and renew existing ones.
The measure provides $28.6 billion to address natural disasters like Hurricane Ida which slammed into the Gulf Coast earlier this month, and $6.3 billion to provide resettlement assistance for Afghan refugees fleeing the Taliban. Another $2.5 billion goes toward care and shelter for undocumented migrant children who crossed the border alone while the government reviews their status.
From the telehealth front
- Healthcare Dive reports that
Telehealth usage was four times higher than a year ago, but the industry and patients are still grappling with growing pains including service limitations, difficulty accessing appointments and inconsistent care, a survey from J.D. Power found.
From 2020 to 2021, overall satisfaction with both direct-to-consumer and payer-sponsored telehealth services declined, according to the survey. Patients frequently cited limited services, lack of awareness of costs and confusing technology requirements.
Among direct-to-consumer brands, Teladoc ranked highest for telehealth satisfaction, followed by MDLive. Among payer-sponsored telehealth services, UnitedHealthcare ranked the highest, followed by Humana and Kaiser Foundation Health Plan, both in a tie for second, the survey found.
- STAT News tells us that
Despite the wide-ranging expansion of telehealth in the past year, there is still a broad swath of the U.S. population it has largely failed to reach: the 57 million people in rural parts of the country.
Even now, as employers rush to add virtual care to their benefits, many telehealth companies have avoided rural areas. Several acknowledged to STAT that most of their users remain in urban and suburban areas, and they’ve made far less progress than they’d like to in reaching rural patients. The companies recognize they face an uphill battle. Beyond the foundational barrier of broadband access, providers must contend with questions about reimbursement rates, strict rules on interstate licensing, and a hazy road map without clear inroads for reaching rural patients and providers.
“Honestly, as much as our mission statement fits well with rural health care, we haven’t really made enough progress to date around this work,” Brad Younggren, the chief medical officer of telehealth company 98point6, told STAT.
As it is Thursday from the miscellany department
- Recycle Intelligence discusses “Lessons learned from Aetna, Cleveland Clinic’s Joint ACO Mode / Leaders from Aetna and Cleveland Clinic reflect on the first year of their joint ACO and health plan and share how others can deliver value-based care to their local markets.” Check it out.
- STAT News informs us that
Scientists have unveiled new maps of the protein networks underlying different types of cancer, offering a potentially clearer way to see what’s driving the disease and to find therapeutic targets.
Sequencing the genetic information of tumors can provide a trove of data about the mutations contained in those cancer cells. Some of those mutations help doctors figure out the best way to treat a patient, but others remain more of a mystery than a clear instruction manual. Many are exceedingly rare, or there are so many mutations it’s not clear what’s fueling the cancer.
In a quest to come up with more practical and actionable tools, experts have been looking beyond the genes. Instead, they’re mapping out the proteins the genes encode and the interactions among those proteins in hopes of getting a clearer view of cancer-propelling pathways. And in a series of papers published Thursday in the journal Science, a team of researchers outlined those “protein-protein interaction” maps for certain cancers and explain how charting those landscapes and others like them could reveal insights about patients’ prognoses, point to drugs to try for particular patients, and perhaps identify targets for new therapies.
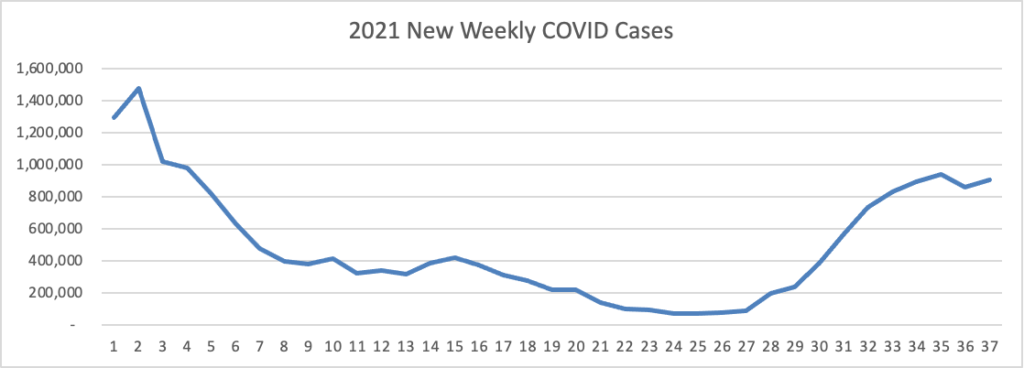
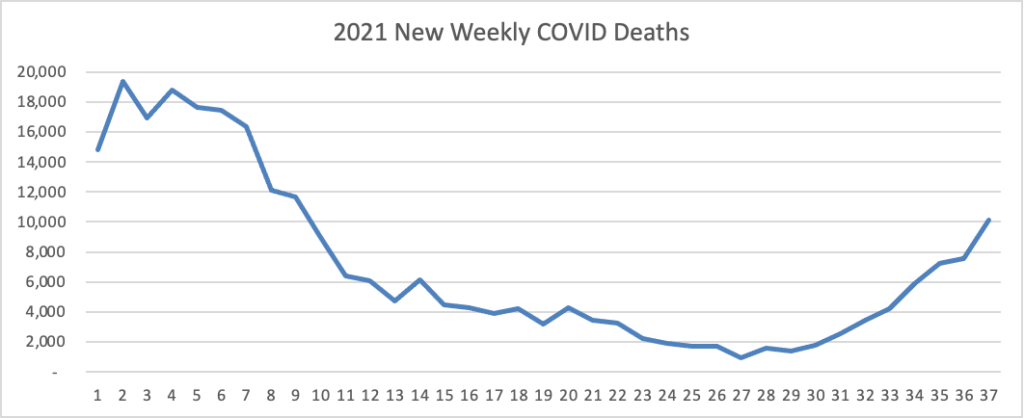
- STAT News also seeks to predict what will become of the COVID pandemic this coming winter. The article hopefully concludes
Barney Graham, who led the vaccine design work that laid the foundation for many of the current Covid vaccines, is hopeful, though, that in Delta the virus has hit a sweet spot that will eventually undermine it.
“I’m hoping the virus has gotten itself to a point where it’s basically trapped now,” said Graham, who was deputy director of the NIH’s Vaccine Research Center until his retirement at the end of August. “That it can’t get any better at transmission, and any adaptation it makes in the immune response is going to make it less transmissible.”
- In support of this optimism, Reuters reports that
Laboratory studies show that Merck & Co’s (MRK.N) experimental oral COVID-19 antiviral drug, molnupiravir, is likely to be effective against known variants of the coronavirus, including the dominant, highly transmissible Delta, the company said on Wednesday.
Since molnupiravir does not target the spike protein of the virus – the target of all current COVID-19 vaccines – which defines the differences between the variants, the drug should be equally effective as the virus continues to evolve, said Jay Grobler, head of infectious disease and vaccines at Merck.
Molnupiravir instead targets the viral polymerase, an enzyme needed for the virus to make copies of itself. It is designed to work by introducing errors into the genetic code of the virus.
Data shows that the drug is most effective when given early in the course of infection, Merck said.
What’s more, the Merck drug is administered in pill form.