The CDC’s Advisory Committee on Immunization Practices will take up the FDA’s grant of emergency use authorization to the Novovax traditionally developed Covid vaccine tomorrow.
The American Hospital Association tells us “Two doses of the Pfizer or Moderna COVID-19 vaccine were less effective at preventing hospitalizations during the omicron BA.2 and BA.2.12.1 periods than during the BA.1 period, but a third and fourth dose provided additional protection to eligible adults, the Centers for Disease Control and Prevention reported Friday.”
“Getting vaccinated now will not prevent you from getting an authorized variant-specific vaccine in the fall or winter when they are recommended for you,” CDC said. “Given recent increases in deaths and hospitalizations associated with the BA.5 variant, everyone should stay up to date with recommended COVID-19 vaccinations, including additional booster doses for those who are moderately to severely immunocompromised and adults over 50.”
Also from the public health front, Medscape reports
Iron accumulation in the brain as a result of alcohol consumption may explain why even moderate drinking is linked to compromised cognitive function.
Results of a large observational study suggest brain iron accumulation is a “plausible pathway” through which alcohol negatively affects cognition, study Anya Topiwala, MD, PhD, senior clinical researcher, Nuffield Department of Population Health, University of Oxford, Oxford, England, told Medscape Medical News.
Study participants who drank 56 grams of alcohol a week had higher brain iron levels. The UK guideline for “low risk” alcohol consumption is less than 14 units weekly or 112 grams.
Research supported by the National Institutes of Health shows that cardiovascular-related deaths have declined over the past two decades, but disparities remain. Researchers found that inequities are mostly driven by differences in race and ethnicity, geographic location, and access to care, among other factors. The findings were published in Circulation, and the research was partially funded by the National Heart, Lung, and Blood Institute (NHLBI), part of NIH.
In one paper(link is external), researchers analyzed data from the Centers for Disease Control and Prevention and found that, after adjusting for age, rates of cardiovascular disease-linked deaths dropped among Black and white adults between 1999 and 2019, as did heart disease-related disparities between the two groups. However, Black adults continue to experience higher death rates than white adults, especially in rural or segregated areas, according to the researchers.
From the Medicare front, Healthcare Dive informs us
Federal health regulators want to increase hospital outpatient payments by 2.7% for 2023, an increase of about $6.2 billion in Medicare payments from this year.
Yet, the American Hospital Association is “deeply concerned” about the proposed Medicare payment rate amid increased inflation.
“A much higher update is warranted,” AHA Executive Vice President Stacey Hughes said in a Friday statement following the release of the proposed 2023 Hospital Outpatient Prospective Payment System rule.
Circular logic, like the AHA’s here, feeds inflation in the FEHBlog’s view.
From the U.S. healthcare business front, MedPage Today reports “A growing demand for specialty services is once again spurring a bump in starting salaries for specialty physicians, according to a new report from AMN Healthcare and its physician search division, Merritt Hawkins. ‘Demand for physicians, and the salaries they are offered, have rebounded dramatically from the height of COVID-19,’ AMN’s president of physician permanent placement, Tom Florence, said in a statement. ‘Virtually every hospital and large medical group in the country is looking to add physicians.'”
From the health insurance literacy front, Benefits Pro observes
Despite spending more than $1 trillion on health insurance each year, many U.S. consumers are making poorly informed decisions – and paying for their lack of understanding.
According to the latest Health Insurance Literacy Survey from HealthCare.com:
* 1 in 4 Americans say lack of health insurance understanding caused them to receive a higher-than-expected medical bill.
* Half believe that copays count toward deductibles when they generally do not.
* Half of the respondents say they can’t afford health insurance without employer coverage.
* 3 in 10 stay in jobs they don’t like or take jobs they don’t want so they can receive health insurance.
The survey of 1,000 consumers younger than 65 identified several broad areas of concern, including confusion and complexity and unfounded confidence.
The Wall Street Journal reported last Friday evening
President Biden signaled he was prepared to support a narrow bill that lowered prescription drug costs and extended Affordable Care Act subsidies but left out climate provisions, as Senate Democrats grappled with whether to abandon their broader economic agenda after intraparty talks hit an impasse.
Mr. Biden said that if the Senate didn’t move forward with climate legislation, he would turn to executive action, calling clean energy and combating climate change urgent matters. On the prescription drug portion of the agenda, he said the Senate “should move forward, pass it before the August recess, and get it to my desk so I can sign it,” characterizing it as a major victory for American households.
The statement came a day after talks between Sen. Joe Manchin (D., W.Va.) and Senate Majority Leader Chuck Schumer (D., N.Y.) broke down. Mr. Manchin told Mr. Schumer that he would back a prescription-drug proposal but couldn’t yet commit to backing tax increases or climate provisions, citing inflation worries.
The BA.5 omicron subvariant, which is now the most prevalent coronavirus strain in the United States, is four times more resistant to COVID-19 vaccines, according to a new study.
The strain, which is considered “hypercontagious,” according to the Mayo Clinic, is more defiant against messenger RNA vaccines, which include Pfizer and Moderna.
The BA.5 strain represented 65% of cases from July 3 to 9, according to data from the Centers of Disease Control and Prevention.
It is contributing to increases in COVID-19 hospitalizations and admissions to intensive care units across the country.
But vaccines still provide much better protection than going without the safeguards.
Bloomberg Prognosis adds
Bertha Hidalgo, a University of Alabama epidemiologist, was faked out by a variant that never truly got off the launchpad.
“A few weeks ago, I thought BA2.12.1 would drive the summer wave and it would be a small wave, with not too many infections, to be followed by a BA.5 wave when schools reopened,” she says.
Instead, the BA.5 omicron variant decided that the summer of 2022 was its time to shine. The variant is now dominant in the US, according to the Centers for Disease Control and Prevention. Combined with BA.4, it is also powering a surge of the virus in Europe.
This week, World Health Organization chief Tedros Adhanom Ghebreyesus warned that “new waves of the virus demonstrate again that Covid-19 is nowhere near over.”
The good news is that we now know much more about what strategies are effective for reducing spread of the virus as we go about our lives in these very odd times.
Hidalgo shared her list of best practices:
* Get vaccinated and get all available boosters
* Wear a mask indoors (and outdoors if in crowded spaces)
* Make sure to get a good quality, good fitting mask, like a KN95
* Use rapid tests before gathering with others, or at the sign of any questionable symptoms
* If gathering indoors, consider improving ventilation through measures like opening windows or running a central HVAC system
“All of these are layers of protection we can take advantage of that are preventive and can help reduce chances of infection and transmission,” she says.
Quite honestly, the FEHBlog relies on vaccines, including boosters, and rapid tests along with common sense.
Until now, the commission took the position that the Americans with Disabilities Act standard for medical examinations always permitted employer worksite COVID-19 testing.
Going forward, employers will need to assess whether current pandemic circumstances and individual workplace circumstances justify testing to prevent workplace transmission, the agency said. Specifically, an employer must show that testing is job-related and consistent with business necessity, as defined by the ADA.
From the unusual viruses front, Govexec brings us a CDC update on monkeypox. Here are links to
From the U.S. healthcare business front, Fierce Healthcare offers 21st Century advice on improving health plan call centers.
From the mental healthcare front, NPR takes a deep dive into the new 988 suicide and mental health crisis number.
From the HIPAA privacy and security rule enforcement front, HHS’s Office for Civil Rights announced “the resolution of eleven investigations in its Health Insurance Portability and Accountability Act (HIPAA) Right of Access Initiative, bringing the total number of these enforcement actions to thirty-eight since the initiative began. OCR created this initiative to support individuals’ right to timely access their health records at a reasonable cost under the HIPAA Privacy Rule.” All of the chastised parties were healthcare providers.
This morning the FEHBlog was doing his weekly quality review of the FEHBlog. He noticed that last Thursday, he mentioned a new Kaiser Family Foundation report without providing a topic or a link for his readers. Lo siento. Here is the missing information:
Pregnancy is one of the most common reasons for a hospitalization among non-elderly people. In addition to the cost of the birth itself, pregnancy care also involves costs associated with prenatal visits and often includes care to treat psychological and medical conditions associated with pregnancy, birth, and the post-partum period.
This analysis examines the health costs associated with pregnancy, childbirth, and post-partum care using a subset of claims from the IBM MarketScan Encounter Database from 2018 through 2020 for enrollees in large employer private health plans. It finds that health costs associated with pregnancy, childbirth, and post-partum care average a total of $18,865 and the average out-of-pocket payments total $2,854. The analysis also examine how pregnancy, childbirth, and post-partum health spending among large group enrollees varies by the type of delivery.
The analysis can be found on the Peterson-KFF Health System Tracker, an information hub dedicated to monitoring and assessing the performance of the U.S. health system.
Childbirth also is one of the required out-of-pocket cost requirements for a health plan’s ACA summary of benefits and coverage template.
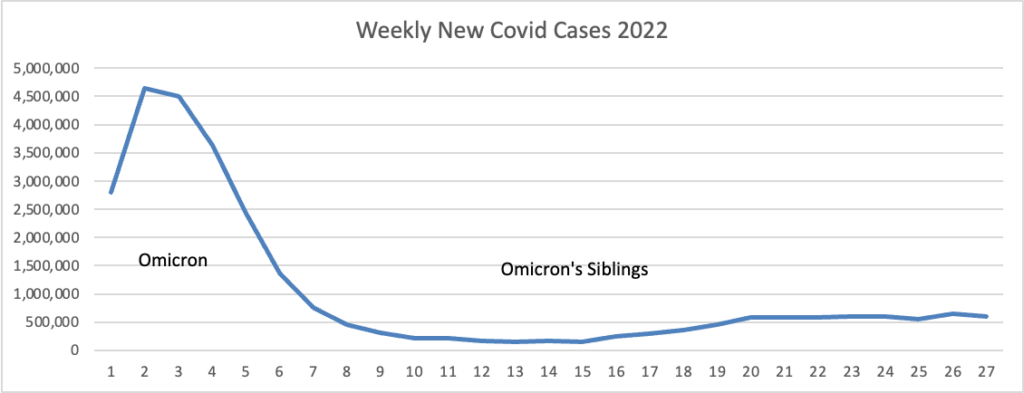
Based on the CDC’s Covid Data Tracker and using Thursday as the first day of the week, here is the FEHBlog’s weekly chart of new Covid cases for this year:
The CDC’s weekly review of its Covid statistics adds
As of July 13, 2022, the current 7-day moving average of daily new cases (124,048) increased 15.7% compared with the previous 7-day moving average (107,174).
CDC Nowcast projections* for the week ending July 9, 2022, estimate that the combined national proportion of lineages designated as Omicron will continue to be 100% with the predominant Omicron lineage being BA.5, projected at 65.0% (95% PI 62.2-67.7%).
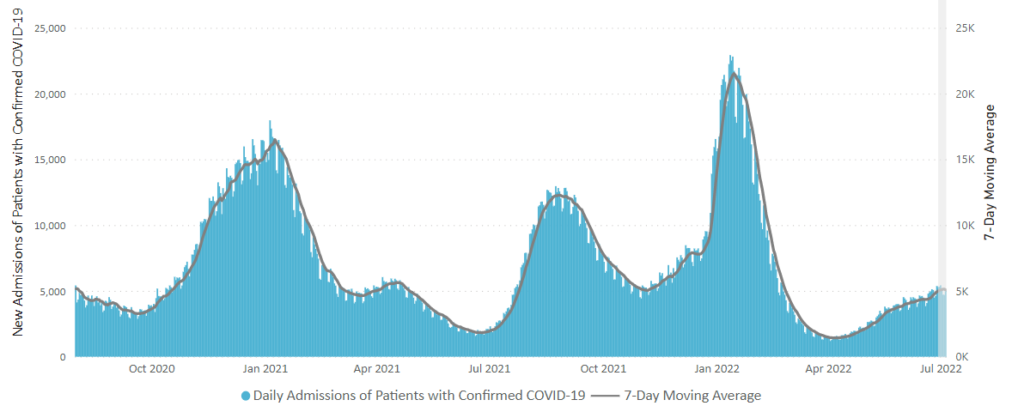
Here is the CDC’s chart of daily trends in new Covid hospital admissions:
The CDC’s weekly review adds “The current 7-day daily average for July 6–12, 2022, was 5,851. This is a 14.4% increase from the prior 7-day average (5,115) from June 29–July 5, 2022.”
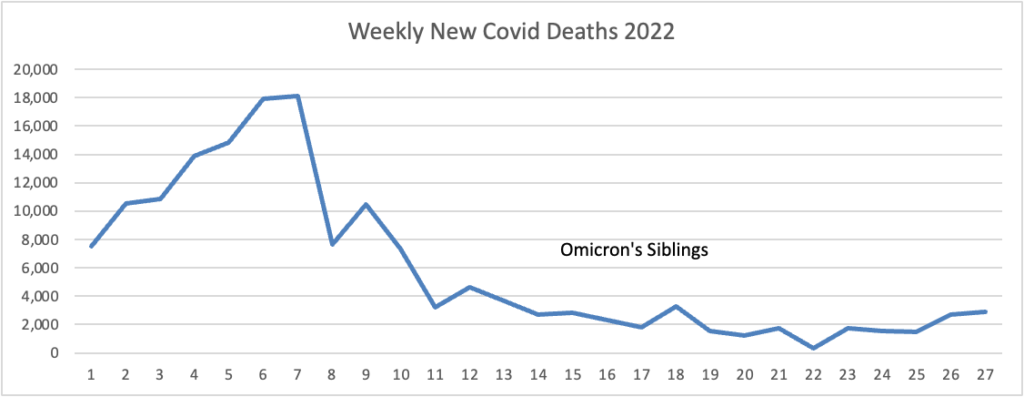
Here’s the FEHBlog’s weekly chart of new Covid deaths for 2022: “The current 7-day moving average of new deaths (352) has increased 12.6% compared with the previous 7-day moving average (312).”
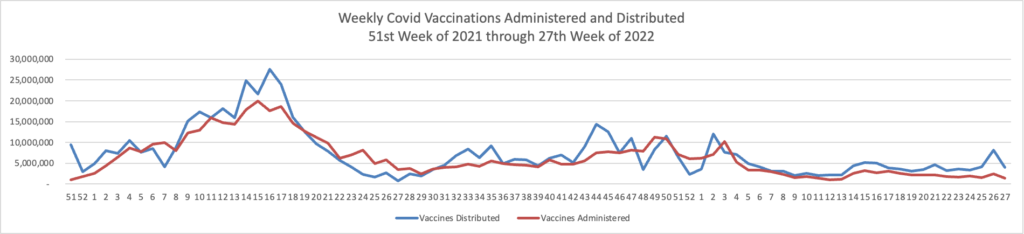
Here’s the FEHBlog’s weekly chart of Covid vaccinations distributed and administered:
The CDC’s weekly review adds
Overall, about 260.7 million people, or 78.5% of the total U.S. population, have received at least one dose of vaccine. About 222.7 million people, or 67.1% of the total U.S. population, have been fully vaccinated.* Of those fully vaccinated, about 107.0 million people have received a booster dose,** but 50.2% of the total booster-eligible population has not yet received a booster dose. Here’s another visual breakdown, this time from the CDC
The CDC’s weekly review summarizes the situation as follows:
As of July 14, 2022, there are 1,141 (35.4%) counties, districts, or territories with a high COVID-19 Community Level, 1,275 (39.6%) counties with a medium Community Level, and 804 (25.0%) counties with a low Community Level. Compared with last week, this represents an increase (+14.8 percentage points) in the number of high-level counties, an increase (+1.8 percentage points) in the number of medium-level counties, and a corresponding decrease (−16.4 percentage points) in the number of low-level counties. 50 out of 52 jurisdictions* had high- or medium-level counties this week. Rhode Island and Maine are the only jurisdictions to have all counties at low Community Levels.
The American Hospital Association informs us “The Department of Health and Human Services today renewed the COVID-19 public health emergency declaration for another 90 days. The AHA and other national health care organizations have urged HHS to maintain the public health emergency until it’s clear that the global pandemic has receded and the capabilities authorized by the PHE are no longer necessary.” In that event, the Covid PHE may never end. Here’s the rub :
[T]he additional 6.2% in Federal Medical Assistance Percentage funding for the state Medicaid programs, designated in the Families First Coronavirus Relief Act, is tied to the length of the PHE and the continuous coverage requirement has been essential in helping provide health care coverage to vulnerable populations during the economic downturn.
KFF provides context “After declines in enrollment from 2017 through 2019, preliminary data for March 2022 show that total Medicaid/CHIP enrollment grew to 87.9 million, an increase of 16.7 million from enrollment in February 2020 (23.4%), right before the pandemic and when enrollment began to steadily increase.”
The FEHBlog is not suggesting cutting back Medicaid. The FEHBlog is suggested that Congress decouple these important actions from the PHE period.
From the Medicare front, the American Hospital Association informs us
The Centers for Medicare & Medicaid Services late today issued a proposed rule that would increase Medicare hospital outpatient prospective payment system rates by a net 2.7% in calendar year 2023 compared to 2022.
In a statement shared with the media, AHA Executive Vice President Stacey Hughes said, “We are deeply concerned about CMS’ proposed payment update of only 2.7%, given the extraordinary inflationary environment and continued labor and supply cost pressures hospitals and health systems face … A much higher update is warranted, and we will be closely analyzing CMS’ proposed market basket, as well as its proposed productivity offset.”
From the Rx coverage front, Healthcare Dive informs us
UnitedHealth plans to offer some medicines at zero cost share to eligible members in 2023, including insulin and other emergency-use drugs, in a bid to address inflationary pressures and keep patients out of the emergency room, CEO Andrew Witty announced.
The offering from the Minnetonka, Minnesota-based company, which operates the largest private payer in the U.S., applies to UnitedHealth’s standard insured group plans. But the larger cost containment of drugs must come from pharmaceutical manufacturers lowering prices, Witty told investors during UnitedHealth’s second-quarter earnings call on Friday.
UnitedHealth beat Wall Street expectations for earnings and revenue in the quarter with revenue of $80.3 billion, up 13% year over year. Profit of $5.2 billion was up 19% year over year. UnitedHealth increased its full-year earnings expectations on the results.
With new competitors closing in, UnitedHealth is bolstering its defenses by purchasing Genoa Healthcare, the fifth-largest pharmacy chain in the country with 435 locations. Genoa—which also offers telepsychiatry services and medication management for behavioral health patients—will be absorbed by UnitedHealth’s pharmacy benefit manager OptumRx. According to its website, Genoa fills more than 15 million prescriptions each year and serves more than 650,000 customers.
From the telehealth front, OPM’s chief medical officer Dr. Ron Kline issued a newsletter to FEHB carriers on the topic of telehealth.
From the transparency front, Fierce Healthcare tells us
Major health insurers have released massive reams of data detailing their in- and out-of-network rates to comply with a new rule.
Now, experts are sifting through those data to identify trends that could affect contract negotiations with providers.
“So far so good, if you will, on compliance,” said Niall Brennan, chief analytics and privacy officer for Clarify Health, a healthcare analytics software company. “I don’t have a truly overarching picture right down to the smallest plans, but so many of the nationals and [Blue Cross plans] are participating. Even if some of the smaller plans are a little slower … we are probably catching the vast majority of rates.”
Third parties are now looking into how to use the data that have been released, which is a tall order.
“The amount of data is massive,” said Marcus Dorstel, vice president of operations at Turquoise Health, which has created a consumer website to compare prices for hospitals.
West Virginia Democrat Joe Manchin III is yet again upending his party’s priority economic package, jettisoning climate measures and tax increases he previously favored and leaving only provisions focused on lowering health care costs.
Manchin communicated the decision to his negotiating partner, Senate Majority Leader Charles E. Schumer, on Thursday, according to two Democratic sources familiar with the situation.
The move came one day after Manchin expressed heightened anxiety about inflation, after the June consumer price index data released that morning showed inflation climbed 9.1 percent on an annualized basis over the previous year.
The House on Thursday passed, 329-101, its version of the fiscal 2023 National Defense Authorization Act, which would authorize $840.2 billion in national defense spending, after sifting through hundreds of amendments and hours of debate.
The sprawling Pentagon policy bill, which has been enacted into law every year for the past 61 years, would authorize funds for the Defense Department and national security programs within the Department of Energy. * * *
In the coming months, the Senate will take up its own version of the annual defense policy bill.
This must-pass bill typically includes significant federal procurement changes that can impact FEHB contracts.
From the Omicron and siblings front, MedPage Today offers an expert opinion on whether to get a second Covid booster or wait until the fall for potentially improved Covid shots?
For those still deciding, the CDC’s booster calculator provides guidance for anyone unsure about their eligibility. Generally speaking, for people age 60 and older, a first booster is recommended for those who received primary immunization more than 5 months previously, and a second booster is recommended for those who received their first booster more than 4 months ago.
James Grisolia, MD, a San Diego neurologist, described it as a physician’s dilemma. “While we were between surges, I would have given similar advice (to wait before getting the second booster) but as of several weeks ago, it was obvious we were going into another surge. I began encouraging older folks to get their second booster.”
From the FEHB front —
Fedweek discusses the differences in levels of FEHB coverage.
Benefits consultant Tammy Flanagan wraps up her three-part series on one federal employee’s journey into retirement with an article on FEHB issues.
From the telehealth front, Healthcare Dive offers an interview with Teladoc’s chief medical officer, Vidya Raman-Tangella.
From the mental healthcare front, here is a link to SAMHSA’s 988 nationwide suicide/mental healthcare crisis hotline which becomes available on Saturday, July 16.
From the reports department
CVS Health released its Health Care Insights 2022 report.
The Kaiser Family Foundation issued a report on the cost of delivering a baby in the U.S. “This analysis examines the health costs associated with pregnancy, childbirth, and post-partum care using a subset of claims from the IBM MarketScan Encounter Database from 2018 through 2020 for enrollees in large employer private health plans. It finds that health costs associated with pregnancy, childbirth, and post-partum care average a total of $18,865 and the average out-of-pocket payments total $2,854.”
From the U.S. healthcare business front, MedPage Today identifies the largest physician groups in our country.
Novavax’s product is a protein subunit vaccine that contains the SARS-CoV-2 spike protein plus an adjuvant to enhance the recipient’s immune response. The product is to be administered as a two-dose primary series given 3 weeks apart.
Becker’s Hospital Review discusses the White House’s latest Covid strategy.
From the No Surprises Act front, the U.S. Office of Personnel Management issued a carrier letter today on various NSA topics affecting FEHB carriers.
From the Rx coverage front
The Institute for Clinical and Economic Review (ICER) today released a Draft Evidence Report assessing the comparative clinical effectiveness and value of subcutaneous semaglutide (Wegovy, Novo Nordisk), liraglutide (Saxenda, Novo Nordisk), phentermine/topiramate (Qsymia, Vivus Pharmaceuticals), and bupropion/naltrexone (Contrave, Currax Pharma) for the treatment of obesity. This preliminary draft marks the midpoint of ICER’s eight-month process of assessing these treatments, and the findings within this document should not be interpreted to be ICER’s final conclusions.
On July 26, 2022, as part of ICER’s Early Insights Webinar Series, ICER’s Senior Medical Advisor Francesca Beaudoin, MD, PhD, MS will present the initial findings of this draft report. This webinar is exclusively available to all users of the ICER Analytics platform; registration for the webinar is now open.
From the Dobbs front, Healthcare Dive has created a state abortion law tracker and the Department of Human Resources announced the steps that its agencies have taken to protect reproductive rights.
From the research studies department, the National Institutes of Health announced today
The percentage of methadone-involved overdose deaths relative to all drug overdose deaths declined from January 2019 to August 2021, according to a new study. Access to methadone, a medication to treat opioid use disorder, was expanded at the start of the COVID-19 pandemic to allow more patients to take home doses, rather than visit a clinic daily. These data indicate that broader access to treatment was not associated with harms. While drug overdose deaths both with and without methadone increased in the month of March 2020, overdose deaths that did not involve methadone continued to increase in the months after the policy changes, while overdose deaths involving methadone held steady.
Published today in JAMA Psychiatry, this study was a collaborative effort led by researchers at the National Institute on Drug Abuse (NIDA), part of the National Institutes of Health, and the National Center for Injury Prevention and Control, part of the Centers for Disease Control and Prevention.
House Rep. Lloyd Doggett, D-Texas, introduced the Assuring Medicare’s Promise Act on Monday aimed at redirecting income tax revenue as a solution to Medicare’s hospital fund that will run out of money in 2028. * * *
The legislation aims to close the loophole for wealthy individuals to bypass paying net investment income tax (NIIT) and would direct the revenue to the Hospital Insurance Fund, which pays for Medicare Part A that covers inpatient care in hospitals. * * *
If the bill is implemented, Doggett expects Medicare Trust Fund solvency to be extended through 2040.
The legislation comes as Congress is taking a sharper eye at ways to shore up Medicare’s finances. The Senate, for instance, is eyeing closing similar loopholes for NIIT and would extend Medicare solvency for another three years, according to a CNN report.
Senate Democrats are working on a deal to give Medicare the power to negotiate lower drug prices, and the tax provisions could be included.
From the Omicron and siblings front, we have mixed bag Covid news from the Wall Street Journal.
Covid-19 is circulating widely as the BA.5 Omicron subvariant elevates the risk of reinfections and rising case counts, spoiling chances for a summer reprieve from the pandemic across much of the U.S.
Covid-19 levels are high in a fifth of U.S. counties, according to the Centers for Disease Control and Prevention’s metric based on case and hospital data, a share that has been mostly rising since mid-April. BA.5 is estimated to represent nearly two in three recent U.S. cases that are averaging just more than 100,000 a day, CDC data show. The true number of infections may be roughly six times as high, some virus experts said, in part because so many people are using at-home tests that state health departments largely don’t track. * * *
The pace of hospital admissions for Covid-19-positive patients has recently sped up, federal data indicate. The seven-day moving average for confirmed Covid-19 patients in hospitals has topped 34,000, federal data show, up from a low near 10,000 in April but far below January’s record peak topping 150,000.
Many of the hospitalizations are cases where patients test positive after being admitted for other reasons. Deaths are hovering around 300 to 350 a day, Dr. Jha said Tuesday. This is much closer to historic lows than highs, though he called the current level unacceptable.
The reduced threat is one reason a pandemic-fatigued populace is less likely to change behavior when cases are high, said Robert Wachter, chairman of the department of medicine at the University of California, San Francisco. * * * “Part of what motivated people to be super careful for a long time was the fear that I’m going to die of this thing,” Dr. Wachter said. “I think people have less fear of that, and that’s not inappropriate.”
From the U.S. healthcare business front
MedPage Today identifies the heavy hitters in Healthcare who topped the recently announced Fortune 500.
Insurance News Net reports that “Commercial health insurers suffered a 90% decrease in underwriting income last year as fewer people signed onto group health and instead moved into individual coverage on an exchange or a Medicaid program, and COVID care requirements far exceeded expectations. * * * Large, diversified carriers fared best, according to Antonietta Iachetta, AM Best senior financial analyst. “Smaller carriers with concentrations in the commercial business found themselves in an especially difficult position — more than half of insurers with capital and surplus under $50 million posted underwriting losses in 2021, the highest share of companies with losses for that group since 2012,” Iachetta said.”
Beckers Payer Issues reviews the history of Mark Cuban’s PBM Cost Plus Drug Co. to identity barriers to competing in that market.
Fierce Healthcare tells us, “Optum has quietly teamed with Red Ventures on a new joint venture focused on consumer health. The venture, called RVO Health, covers a mix of assets from both parties, including Optum’s Store and Perks and Red Ventures’ Healthline Media and Healthgrades. Virtual coaching platforms Real Appeal, Wellness Coaching and QuitForLife, news first reported by Axios. Through these elements, RVO includes a slew of consumer offerings, including doctor ratings through Healthgrades, medical information and communications from Healthline, Optum Perks’ prescription savings card and home delivery of health and wellness products through Optum Store.”
From the U.S. healthcare front
The American Hospital Association reports
After declining in recent years, antimicrobial-resistant infections starting during hospitalization grew 15% from 2019 to 2020, the Centers for Disease Control and Prevention reported today, based on limited data for 2020.
“During the pandemic, hospitals experienced personal protective equipment supply challenges, staffing shortages, and longer patient stays,” the agency notes. “Hospitals also treated sicker patients who required more frequent and longer use of medical devices like catheters and ventilators. The impact of the pandemic likely resulted in an increase of healthcare-associated, antimicrobial-resistant infections.”
More than 90% of U.S. hospitals in 2020 had an antibiotic stewardship program aligned with CDC’s Core Elements of Hospital Antibiotic Stewardship, CDC said. The AHA released an antibiotic stewardship toolkit in 2014 to help hospitals and health systems enhance their antimicrobial stewardship programs based on the CDC’s core elements, and in 2017 partnered with CDC on guidance to help small and critical access hospitals implement programs to improve antibiotic prescribing and use and reduce the threat of antibiotic-resistant infections. For more AHA resources to promote the appropriate use of medical resources, click here.
The CDC’s July 2022 Diabetes Insider called attention to its Diabetes and Your Skin website.
From the mental healthcare front, an expert contributor to HR Morning expresses his views on what employees want in mental health coverage from their employer-sponsored health plans.
From the artificial intelligence front, the Journal of AHIMA looks at the administrative cost savings potential of artificial intelligence.
BA.2.75 is the latest omicron relative catching experts’ attention, with three cases recently identified on the West Coast, Timereported July 11.
Two cases were detected in California and one in Washington as of July 8, according to data from Helix, which works with the CDC on viral surveillance.
The subvariant is gaining traction in India and has also been detected in 10 other countries.
Better start looking over your shoulders Omicron subvariants BA.4 and BA.5.
Moderna Inc. said it is developing two potential Covid-19 booster shots targeting different Omicron subvariants, citing differences in market preferences among the U.S. and other countries.
The Cambridge, Mass., company said Monday it has completed requests for regulatory authorization of one of its new booster shots in the European Union, the U.K. and Australia. The company expects to complete regulatory filings elsewhere this week.
In these countries, Moderna is seeking authorization for the use of mRNA-1273.214, a vaccine that targets both the ancestral strain of the coronavirus and the BA.1 subvariant of Omicron. The BA.1 subvariant was predominant earlier in the year but has been largely displaced by other Omicron subvariants in many countries.
In the U.S., however, Moderna will develop a different dual-target booster, mRNA-1273.222, which goes after both the ancestral strain and the BA.4 and BA.5 subvariants of Omicron. These subvariants, which are nearly identical to each other for the purposes of a vaccine, now account for most new cases of Covid-19 in the U.S.
What about BA.2.75?
An announcement from HHS today points to an FDA emergency use authorization of the traditionally developed Novovax in the near future.
The U.S. Department of Health and Human Services (HHS), in collaboration with the Department of Defense (DOD), today announced that it has secured 3.2 million doses of Novavax’s COVID-19 vaccine. The protein-based, adjuvanted vaccine will be made available for free to states, jurisdictions, federal pharmacy partners, and federally qualified health centers if it receives U.S. Food and Drug Administration (FDA) Emergency Use Authorization (EUA), and recommendation from the Centers for Disease Control and Prevention (CDC). The company is expected to complete all necessary quality testing in the next few weeks, which would support final release of the product.
Treatment with oral sabizabulin (Veru Pharmaceuticals) cut the risk for death by more than 55% in hospitalized patients with COVID-19, an interim analysis of a phase 3 placebo-controlled trial found.
Sabizabulin treatment consistently and significantly reduced deaths across patient subgroups “regardless of standard of care treatment received, baseline WHO scores, age, comorbidities, vaccination status, COVID-19 variant, or geography,” study investigator Mitchell Steiner, MD, chairman, president, and CEO of Veru, said in a news release.
The company has submitted an emergency use authorization request to the US Food and Drug Administration to use sabizabulin to treat COVID-19.
Sabizabulin, originally developed to treat metastatic castration-resistant prostate cancer, is a novel, investigational, oral microtubule disruptor with dual antiviral and anti-inflammatory activities. Given the drug’s mechanism, researchers at Veru thought that sabizabulin could help treat lung inflammation in patients with COVID-19 as well.
Benefits Pro calls to our attention health plan stop-loss insurer Sun Life’s top 10 high-cost claim conditions report.
Sun Life’s latest report saw a 354% increase in the number of COVID-19 claims from 2020 to 2021 [the Delta variant] —specifically, 107 claims to 486 claims. Total spend also rose from $30.4M to $114.0M, although the average cost for treatment went from $283.7K to $231.2K over the same period, amounting to an 18% decrease. Even so, COVID-19 landed (“somewhat ironically,” the study stated) at number 19 on Sun Life’s top 20 list of high-cost claim conditions over four years. This is significant, as every other condition on the list has amassed four years worth of claims to COVID’s two, underlining the severity of the pandemic.
Two manufacturers of contraceptive pills have been jockeying for FDA clearance to sell their medications over the counter for more than half a decade. Now, against the backdrop of an intense debate over reproductive rights, one of those drugmakers is officially in the running for an approval.
HRA Pharma has applied to the FDA for approval of what could be the first over-the-counter birth control pill in the U.S., the Perrigo-owned company said Monday. The move comes shortly after the Supreme Court’s decision to overturn Roe v. Wade, which has ignited a nationwide clash over reproductive rights.
HRA’s application specifically seeks to convert the prescription approval for the so-called mini pill or non-estrogen pill, dubbed Opill, into an over-the-counter approval.
At the same time, Cadence Health, another maker of birth control pills that’s been in talks with the FDA about converting its med’s approval into an over-the-counter one, said it hopes to move closer to submitting its application in the coming year, The New York Times reports.
FDA approval of OTC contraceptives should have been approved years ago, in the FEHBlog’s opinion.
From the SDOH front, Health Payer Intelligence informs us
The Association for Community Affiliated Plans (ACAP) has initiated a center designed to spur new ideas about how to address social determinants of health, according to a press release that HealthPayerIntelligence received by email.
“Longstanding racial inequities cannot improve without meaningfully addressing the social factors underlying them,” Margaret A. Murray, chief executive officer of ACAP, shared in the press release.
“Safety Net Health Plans have worked in communities across the United States to address factors that shape their members’ health for decades. This new center creates unique opportunities to showcase what works, share that knowledge with others, and support a healthier future for people with low incomes, whose wellbeing has too often been held back by their environment.”
Bravo.
The Wall Street Journal reminds us that the new three-digit 988 suicide hotline launches on Saturday, July 16.
Health officials preparing to broaden the reach of a national mental-health crisis line are working to strengthen an overstretched network of call centers that didn’t connect with about one in six callers in recent years, a Wall Street Journal data review showed.
The National Suicide Prevention Lifeline will transition on July 16 to a three-digit number for calls and texts, 988, from a 10-digit number that has operated since 2005 in coordination with local crisis centers. The line’s operators, including the Substance Abuse and Mental Health Services Administration and the nonprofit Vibrant Emotional Health, said they expect an increase in calls to the shorter and more memorable 988 number during the next year. Stress, suffering and disruption of routines during the pandemic has worsened many people’s mental health, clinicians have said.
Congress returns on Monday with Democrats aiming to revive central pieces of President Biden’s stalled economic agenda while trying to keep on track a separate, bipartisan bill targeted at boosting competitiveness with China that top Republicans are threatening to block.
House Democrats also are set to roll out legislation responding to the Supreme Court ruling ending federal abortion protections. The push could include legislation to write into law the right to an abortion before fetal viability, as well as a bill intended to block any state attempts to criminalize travel for the purpose of getting an abortion. The bills wouldn’t have enough support to pass the Senate.
The three-week work period may be the last chance lawmakers have for a legislative victory before campaigning begins in earnest for midterm election races across the country. Republicans are heavily favored to win back control of the House this fall, while the Senate is seen as a tossup.
From the Omicron and siblings front, MedTecHDive Dive informs us
A single antigen test may only be able to correctly identify the virus 60% of the time in patients who have the omicron variant and who display symptoms of the disease, Tim Stenzel, director of the Food and Drug Administration’s Office of In Vitro Diagnostics and Radiological Health, said during a [recent[ meeting on testing.
The FDA is seeing an increase in samples with the omicron variant that have a relatively low viral load, also referred to as a low positive. “Instead of seeing the usual 10% to 20% low positives in clinical studies last year, we saw a jump to 30% to 40% low positives,” Stenzel said. “When you have 40% low positives… you’re going to see a really big hit in sensitivity.”
The lower sensitivity means people testing for Covid should use multiple antigen tests to rule out a negative result, with 24 to 48 hours between tests, according to the regulator.
From the unusual viruses front, Medpage Today discusses the ties between cases of monkeypox and syphillis.
Syphilis is a known sexually transmitted infection (STI) that can manifest in lesions in the groin area and can transmit through bodily fluid. The genital sores associated with syphilis can make it easier to transmit other diseases such as HIV — and especially pressing at the current moment, genital sores or lesions are also common transmission pathways for the current B1 monkeypox outbreak. While monkeypox has not technically been categorized as an STI, there have been reports of some monkeypox patients also having STIs.
By scaling up testing and treatment for syphilis, we can better identify people who may be more likely to get and transmit monkeypox. Additionally, because the lesions in the genital region can be difficult to distinguish from those associated with syphilis, testing for both conditions is important.
The incidence of syphilis has been increasing in the U.S. In 2020 alone, there were more than 130,000 new cases of syphilis. While 43% of the new infections occur in men who have sex with men, cases have also been rising in heterosexual men and women, and over 50% of the new infections were in people ages 15 to 24.
From the U.S. healthcare front, Fierce Healthcare tells us
Optum is still on an acquisition hot streak, scooping up Healthcare Associates of Texas, Axios reported Wednesday. * * *
HCAT has a large footprint in the Dallas-Fort Worth metropolitan area and has also invested heavily in value-based care, both of which make it an attractive buy for Optum.
Webster bought HCAT in 2016. Neither UnitedHealth nor HCAT has verified the veracity of the deal.
UnitedHealth Group [Optum’s parent] is aiming to address 600 million gaps in care for its members by 2025.
The healthcare and insurance giant released its annual Sustainability Report last week, where it outlined three strategic goals to improve health outcomes and affordability.
Alongside addressing care gaps, the company said it wants to ensure at least 85% of its members receive preventive care each year by 2030 as well as to make sure 55% of outpatient surgeries and radiology services are provided in high-quality, cost-efficient sites of care by 2030.
The CMS’ innovation center has found evidence of implicit bias in three payment models as the agency takes an harder internal look at how its policies might perpetuate health disparities.
The use of certain risk assessment and screening tools, provider processes and payment design algorithms caused some beneficiaries to be unintentionally excluded from the Kidney Care Choices Model, Comprehensive Care for Joint Replacement Model and Million Hearts Cardiovascular Risk Reduction Model, according to a new article published in Health Affairs from Center for Medicare and Medicaid Innovation researchers.
“These findings are troubling” due to limiting access to model participation and stymied efforts to evaluate the models, researchers wrote. CMMI has taken initial steps to address existing bias, and has begun developing a guide to screen and mitigate bias in existing and future models prior to launch, according to the article.
Based on the Centers for Disease Control’s Covid Data Tracker and using Thursday as the first day of the week are the FEHBlog’s weekly charts of new Covid cases for 2022:
The CDC’s Weekly Review of its Covid Statistics observes “As of July 6, 2022, the current 7-day moving average of daily new cases (106,549) decreased 3.9% compared with the previous 7-day moving average (110,875).”
Here is the CDC’s weekly chart of new Covid hospital admissions
The CDC’s Weekly Review comments “The current 7-day daily average for June 29–July 5, 2022, was 5,080. This is a 3.1% increase from the prior 7-day average (4,930) from June 22–28, 2022.”
Here is the FEHBlog’s weekly chart of new Covid deaths for 2022
The CDC’s Weekly review observes “The current 7-day moving average of new deaths (273) has decreased 20.9% compared with the previous 7-day moving average (345).”
Here’s the FEHBlog’s weekly chart of Covid vaccinations distributed and administered from the beginning of the Covid vaccination era in the 51st week of 2020 through the 27th week of 2022.
Overall, about 260.3 million people, or 78.4% of the total U.S. population, have received at least one dose of vaccine. About 222.5 million people, or 67.0% of the total U.S. population, have been fully vaccinated.* Of those fully vaccinated, about 106.6 million people have received a booster dose,** but 50.1% of the total booster-eligible population has not yet received a booster dose.
The American Hospital Association adds
The Food and Drug Administration today granted full approval of Pfizer’s COVID-19 vaccine for young teens, covering the age group spanning 12 to 15 years old. FDA said the vaccine, which has been administered in two-dose regimens to nearly 9 million Americans, earned full approval following its “rigorous analysis and evaluation of the safety and effectiveness data.” The approval does not apply to booster doses for that age group.
The CDC’s Weekly Review also provides the following Communities news:
As of July 7, 2022, there are 666 (20.7%) counties, districts, or territories with a high COVID-19 Community Level, 1,218 (37.8%) counties with a medium Community Level, and 1,331 (41.3%) counties with a low Community Level. Compared to last week, this represents an increase (+1.3 percentage points) in the number of high-level counties, an increase (+2.4 percentage points) in the number of medium-level counties, and a corresponding decrease (−3.7 percentage points) in the number of low-level counties. 49 out of 52 jurisdictions* had high- or medium-level counties this week. Rhode Island, New Hampshire, and Washington, D.C., are the only jurisdictions to have all counties at low Community Levels.
From the Medicare front, Becker’s Hospital Review points out seven things to know about the CMS 2023 Medicare Part B physician payment rule issued yesterday. The lead item has grabbed the medical community’s attention.
The proposed physician fee schedule conversion factor for 2023 is $33.08, down from $34.61 in 2022. The proposal considers a statutory requirement that the conversion factor for 2023 remain flat as well, due to the expiration of the 3 percent increase in physician fee schedule reimbursement payments in 2022 that was required in the Protecting Medicare and American Farmers From Sequester Cuts Act.
For FEHB patients with primary Medicare Part B coverage, this reduction will amount to a cost shift from Medicare to FEHB if implemented by the final rule.
From the No Surprises Act front, Morning Consult offers the results of a survey finding that
One in 5 U.S. adults say they have received an unexpected medical bill this year, according to a new Morning Consult survey that underscores the prevalence of sticker shock in health care — even after federal efforts to combat it.”
The Morning Consult’s survey needs to be taken with a grain of salt because 22% of the surveyed adults are Medicare age (see Survey, p. 131), and the No Surprises Act does not apply to Medicare.
From the Rx coverage front, the PBM’s lobby PCMA compliments the Biden Administration for
taking real action to reduce prescription drug costs. Drug manufacturer pricing strategies that include patent thickets on certain brand drugs unfairly protect those drugs and biologics from generic and biosimilar competition.
The United States Patent and Trademark Office’s and the Food and Drug Administration’s enhanced review power for applications for drug patents that simply don’t deserve an intellectual property extension is a positive step toward eliminating patent thickets and bringing more competition to the marketplace.
That is thoughtful action by the PTO and FDA.
From the Dobbs front, the White House outlines an executive order the President plans to sign in response to the Supreme Court decision.
From the mental health front, Health Payer Intelligence discusses an initiative by “CVS Health and its payer arm, Aetna, [to] expand its existing program with Psych Hub, advancing its efforts around adolescent suicide prevention.” Bravo.
From the artificial intelligence front, the Wall Street Journal reports “Using advanced analytics and AI, health insurers are building targeted medical advice for customers. Now comes the hard part: Getting them to respond. ‘There’s an art to that data communication,’ one doctor says.” Fascinating read.
From the Capitol Hill front, STAT News provides more information on the Senate Democrats’ drug pricing proposal
The text released Wednesday is similar to a sweeping package that passed the House last year — it would allow Medicare to negotiate prices with drugmakers, it would protect seniors from especially exorbitant drug costs, and it would discourage drugmakers from raising their prices dramatically.
There are some notable changes that will affect when patients see savings, how the drug development pipeline works, how certain patients will pay for insulin, and how the new prices would affect safety-net programs and Medicaid.
The Washington Examiner emphasizes The proposal * * * lacks language included in the lower chamber’s bill that would cap insulin prices for people with diabetes at $35 a month.”
Senate Democrats are taking a gamble and removing all of the provisions that would have lowered patients’ insulin prices out of the bill, to allow a separate, bipartisan effort led by Sens. Jeanne Shaheen (D-N.H.) and Susan Collins (R-Maine) to advance.
Now, the HHS secretary would still be allowed to negotiate insulin prices, but only within the parameters and limits of the regular process. Shaheen and Collins’ bill relies on drugmakers voluntarily lowering their prices in exchange for banning rebates for the products.
The brand drug lobby PhRMA blasted the out-of-pocket cost changes, claiming that “Democrats weakened protections for patient costs included in previous versions, while doubling down on sweeping government price-setting policies.”
Six months after regulators issued an emergency use authorization for Paxlovid, physicians say they still have significant questions about prescribing guidelines for the leading treatment for high-risk Covid patients.
STAT spoke with providers who said they and their colleagues aren’t on the same page about when to prescribe Paxlovid or the criteria that separates those who need it from those who do not. They also said it is unclear whether they can give a second course when patients test positive again after taking Paxlovid, a phenomenon known as a rebound. And nearly all the experts who spoke with STAT said that they are clamoring for more data on rebounds, which is complicating and sometimes changing their calculus about when to give the drug.
“There is a real dearth of evidence right now out there, and obviously there’s a lot of confusion,” said Jonathan Li, a physician at Brigham and Women’s Hospital and virology researcher at Harvard Medical School who is also a member of the Covid-19 Treatment Guidelines Panel. “And even amongst people who are immersed in the literature, and who are infectious disease experts, you’ll see actually a fairly wide range in opinions.” * * *
“Pretty much everybody meets the EUA criteria. They made it very, very, very broad,” said David Smith, a professor, physician, and virology researcher at the University of California, San Diego. In a single week in May, over 160,000 Paxlovid prescriptions were filled.
Physicians generally agree that certain high-risk patients — including people who are unvaccinated or those over 65 with multiple comorbidities — should always be prescribed the drug. But the broader eligibility makes it difficult for some physicians to decide who should or should not receive Paxlovid. A child is not likely to need it, but what about a healthy 50-year-old man? A 65-year-old woman? The experts STAT spoke with didn’t agree.
According to Lawrence Kleinman, MD, MPH, of the department of pediatrics at Rutgers Robert Wood Johnson Medical School in New Jersey, we need to take our time in defining long COVID, whether it’s with a checklist, an algorithm, or an entry for the medical dictionary.
“If we defined it a certain way and we missed something in that initial definition, then there will be silence on that until someone comes around and does a postmortem on our analysis,” Kleinman, who is also the lead researcher in the Rutgers pediatric hub of the NIH’s nationwide RECOVER study, told MedPage Today. “We want to avoid that to the extent that’s possible.”
He said more research and data collection are needed before the work of defining long COVID is possible in a clinically meaningful way. At the moment, he noted, there isn’t even clear criteria for where to start.
For example, should researchers focus on setting a specific number of days a person experiences fatigue after an acute COVID infection? If so, what should those ranges look like — fatigue after 30 days? As he pointed out, there are not enough data to develop the foundational elements needed for researchers to piece together a practical definition just yet.
Nothing is simple.
From the Medicare front, the American Hospital Association reports
The Centers for Medicare & Medicaid Services today released its calendar year 2023 proposed rule for the physician fee schedule. The rule proposes to cut the conversion factor to $33.08 in CY 2023, as compared to $34.61 in CY 2022, which reflects the following: the expiration of the 3% statutory payment increase; a 0.00% conversion factor update; and a budget-neutrality adjustment. In addition, CMS proposes to delay for one year (until Jan. 1, 2024) the implementation of its policy to define the substantive portion of a split (or shared) visit based on the amount of time spent by the billing practitioner. Under this policy, if a non-physician practitioner performed at least half of an E/M visit and billed for it, Medicare would only pay 85% of the PFS rate.
CMS proposes numerous policy changes to the Medicare Shared Savings Program. For example, it would modify the manner in which accountable care organizations’ benchmarks are calculated to help sustain long-term participation and reduce costs. It also would provide increased flexibility for certain smaller ACOs to share in savings. The rule also proposes updates to MSSP quality-measurement policies, including a new health equity adjustment that would award bonus points to ACOs serving higher proportions of underserved or dually-eligible beneficiaries.
For the Quality Payment Program, CMS proposes five new, optional Merit-based Incentive Payment System Value Pathways that would be available beginning in 2023. These MVPs align the reporting requirements of the four MIPS performance categories around specific clinical specialties, medical conditions or episodes of care. CMS also proposes refinements to the MIPS subgroup reporting process, an increase to the quality data completeness threshold, and changes to the requirements and scoring of the Promoting Interoperability category. The proposed rule also includes requests for input on policy ideas for advancing health equity and transitioning to digital quality measurement.
The FDA suddenly reversed course this week on its efforts to ban Juul e-cigarette sales, an embarrassing about-face that calls into question the reasoning behind the agency’s initial decision, experts said.
Tuesday evening, the Food and Drug Administration announced it was giving Juul’s application for its vaping products a second look because of “scientific issues … that warrant additional review.” The move came less than two weeks after the FDA made international headlines for ordering all of the vaping giant’s products off the market, prompting praise from lawmakers and advocates alike.
The FDA previously said that Juul “did not provide [sufficient] evidence and instead left us with significant questions,” which prevented the agency from granting its application. But now, it seems, the FDA is acknowledging there is additional information in Juul’s application that regulators didn’t adequately consider.
Fertility benefits and family-building programs have become table stakes for employers looking to support their workforce, but an increasing number of providers and employees are working to offer care during the next stage of reproductive health: menopause.
Nine out of 10 working women said menopause affects their work performance, according to a survey by AARP, which estimates that companies lose $150 billion a year in lost productivity as a result. Yet, 99% of women in the U.S. don’t have access to an employer-sponsored menopause care benefit.
“This is an area that nobody has really focused on, and there isn’t much out there available for employees,” says Maya Bodinger, vice president of business development at P.volve. “The menopause transition can be anywhere from four years to 12. This is not just a year or two like how we traditionally think about reproductive health.”
Cesarean deliveries have increased in the U.S. over the last few years, driven by a rise in patients who underwent first-time C-sections, according to a CDC report.
While the rate of primary C-sections fluctuated from 2016 to 2019, it increased from 2019 to 2021 among women in all age groups, reported Michelle Osterman, MHS, of the CDC’s National Center for Health Statistics.
The repeat cesarean rate, however, which captures patients who have multiple procedures, steadily decreased by around 1% each year from 2016 to 2021 (87.6% to 85.9%), Osterman noted. Repeat cesarean delivery rates decreased specifically for women ages 25 to 39, those who identified as white or Hispanic, and those with full- or late-term pregnancies.
The increase in overall C-sections likely would have been higher if not for the decrease in repeat procedures, she said.
“Because 7 to 9 out of 10 pregnant folks with a prior cesarean will have a repeat cesarean, we can anticipate an overall climb in the overall cesarean delivery rate for the years ahead,” Kjersti Aagaard, MD, PhD, an ob/gyn at Baylor College of Medicine and Texas Children’s Hospital in Houston, told MedPage Today.
Finally, the FEHBlog notes that benefits consultant Tammy Flanagan has released the second part of her three-part story on a typical federal employee’s experience with the federal government’s retirement process. The report appears in Govexec.
We use cookies on our website to give you the most relevant experience by remembering your preferences and repeat visits. By clicking “Accept”, you consent to the use of ALL the cookies.
This website uses cookies to improve your experience while you navigate through the website. Out of these, the cookies that are categorized as necessary are stored on your browser as they are essential for the working of basic functionalities of the website. We also use third-party cookies that help us analyze and understand how you use this website. These cookies will be stored in your browser only with your consent. You also have the option to opt-out of these cookies. But opting out of some of these cookies may affect your browsing experience.
Necessary cookies are absolutely essential for the website to function properly. These cookies ensure basic functionalities and security features of the website, anonymously.
Cookie
Duration
Description
cookielawinfo-checbox-analytics
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Analytics".
cookielawinfo-checbox-functional
11 months
The cookie is set by GDPR cookie consent to record the user consent for the cookies in the category "Functional".
cookielawinfo-checbox-others
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Other.
cookielawinfo-checkbox-necessary
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookies is used to store the user consent for the cookies in the category "Necessary".
cookielawinfo-checkbox-performance
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Performance".
viewed_cookie_policy
11 months
The cookie is set by the GDPR Cookie Consent plugin and is used to store whether or not user has consented to the use of cookies. It does not store any personal data.
Functional cookies help to perform certain functionalities like sharing the content of the website on social media platforms, collect feedbacks, and other third-party features.
Performance cookies are used to understand and analyze the key performance indexes of the website which helps in delivering a better user experience for the visitors.
Analytical cookies are used to understand how visitors interact with the website. These cookies help provide information on metrics the number of visitors, bounce rate, traffic source, etc.
Advertisement cookies are used to provide visitors with relevant ads and marketing campaigns. These cookies track visitors across websites and collect information to provide customized ads.