Congress is on a State / District work break until after Labor Day.
The Change Healthcare antitrust trial is ongoing. The judge Hon. Carl J. Nichols will be deciding the case without a jury. He was heard evidence for ten days already. The case is U.S. v UnitedHealth Group et al., 22-cv-481, U.S. District Court for the District of Columbia.
From the Omicron and siblings front, Bloomberg Prognosis informs us
Scientists fear that the omicron shots coming this fall won’t be all that much better at keeping people from getting Covid than the shots we already have. That’s pushing drugmakers to start working on next-generation vaccines that don’t have to be updated that often, if at all, writes Bloomberg’s Madison Muller, Riley Griffin and Fiona Rutherford.
“Even with the highly flexible platform of mRNA, which is more flexible than virtually anything we’ve had before, it’s going to be very difficult to keep up with the pace of newly evolving variants,” Anthony Fauci, President Joe Biden’s chief medical adviser told Bloomberg. “Which gets us to the question: What about a pan-coronavirus vaccine?”
Aim high.
From the monkeypox front, the World Health Organization has renamed the disease that is quite bland.
Consensus was reached to now refer to the former Congo Basin (Central African) clade as Clade one (I) and the former West African clade as Clade two (II). Additionally, it was agreed that the Clade II consists of two subclades.
A clade means “a group of organisms believed to have evolved from a common ancestor, according to the principles of cladistics, e.g., “the great ape and human clade.” How will WHO distinguish between the monkeypox clade and the chickenpox clade? Time will tell.
From the U.S. healthcare business front, Fierce Healthcare tells us
Humana will acquire a Wisconsin managed care plan in a bid to bulk up its Medicaid services, the insurer announced Friday.
Inclusa, Inc. offers long-term care coverage as well as supporting 16,600 older adults and adults with disabilities in Wisconsin’s Family Care program. The managed care organization has worked with local providers and community resources for more than 20 years to connect members with necessary support and services.
Inclusa partners with more than 6,000 service providers across about 40 service categories, as well as contracts with the state to provide family care services in 68 of Wisconsin’s 72 counties, according to the announcement.
The Wall Street Journal offers two expert interviews on mental health issues:
Speaking of eating, Forbes offers the five best diets for people with diabetes in 2022.
NPR reports on initial experience with the 988 lifelines.
The 988 hotline is the nation’s most comprehensive mental health crisis service and can provide crucial help to those in emotional distress. If you’re thinking about suicide but not taking steps to act on it, 988 is unlikely to call law enforcement without your consent. Instead, 988 counselors can provide resources, referrals and a kind ear. However, if you’re at imminent risk and could act on a plan to kill yourself, police may be called, and you could be taken to a hospital involuntarily.
Sonyia Richardson, a licensed clinical social worker who owns a counseling agency that serves mostly Black and brown clients in Charlotte, N.C., said she didn’t immediately tell her clients about 988 when it launched. Even though she’s a member of her state’s 988 planning committee, she said she needed time to develop trust in the service herself. When she learned at a recent committee meeting that fewer than 5% of 988 calls in North Carolina led to a law enforcement response, she felt reassured.
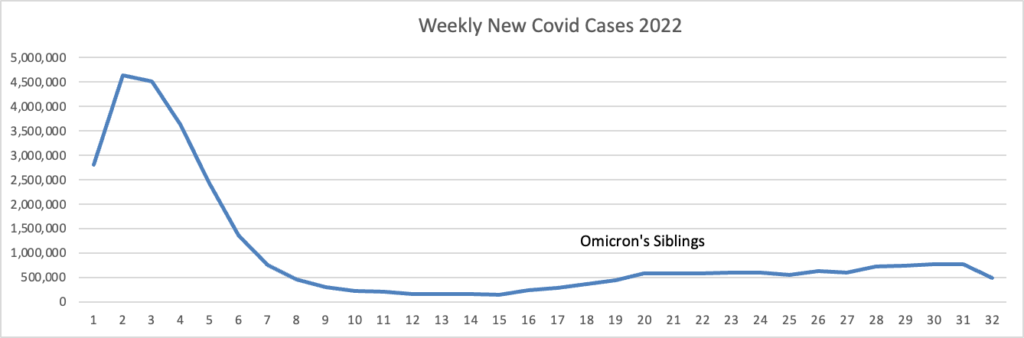
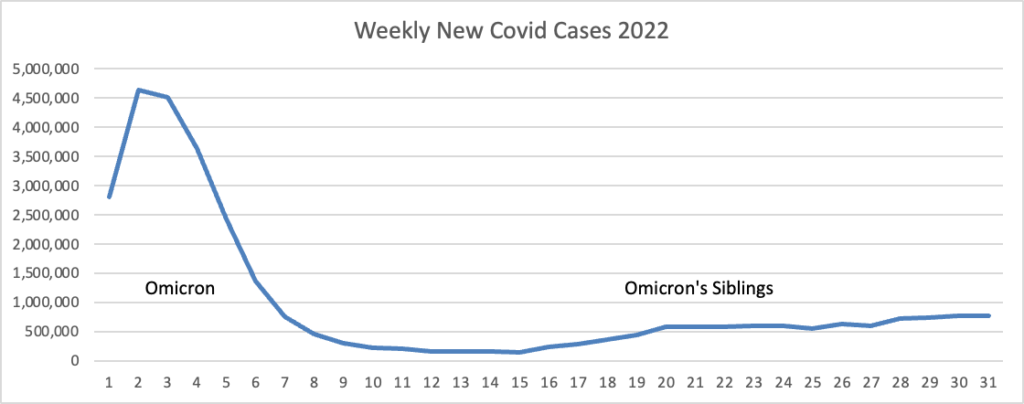
Based on the Centers for Disease Control Covid Data Tracker and using Thursday as the first day of the week, here is the FEHBlog latest weekly chart of new Covid cases:
Note: the massive surge on the left is the original Omicron surge, but the label didn’t carry over from the spreadsheet to the FEHBlog.
The CDC’s weekly review of its Covid statistics tells us
As of August 10, 2022, the current 7-day moving average of daily new cases (103,614) decreased 13.8% compared with the previous 7-day moving average (120,151). * * *
CDC Nowcast projections* for the week ending August 13, 2022, estimate that the combined national proportion of lineages designated as Omicron will continue to be 100% with the predominant Omicron lineage being BA.5, projected at 88.8% (95% PI 87.5-90.0%). The national proportion of BA.4 is projected to be 5.3% (95% PI 4.9-5.7%), BA.4.6 is projected to be 5.1% (95% PI 4.1-6.4%), and BA.2.12.1 is projected to be 0.8% (95% PI 0.7-0.9%).
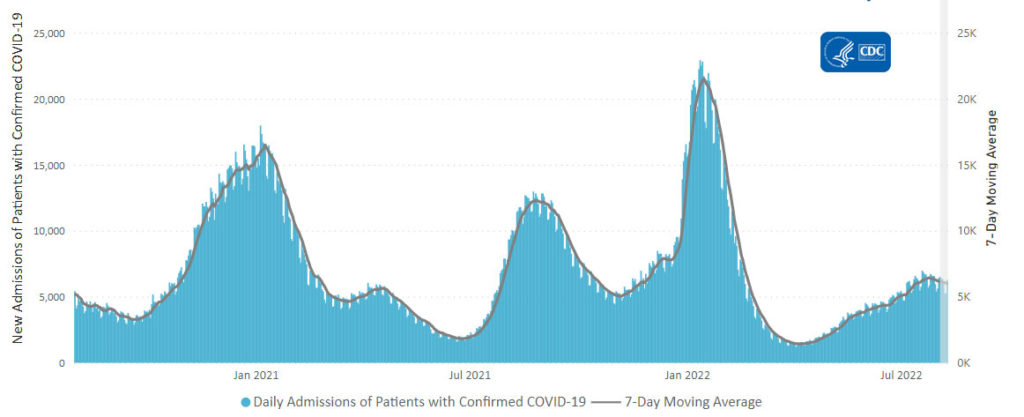
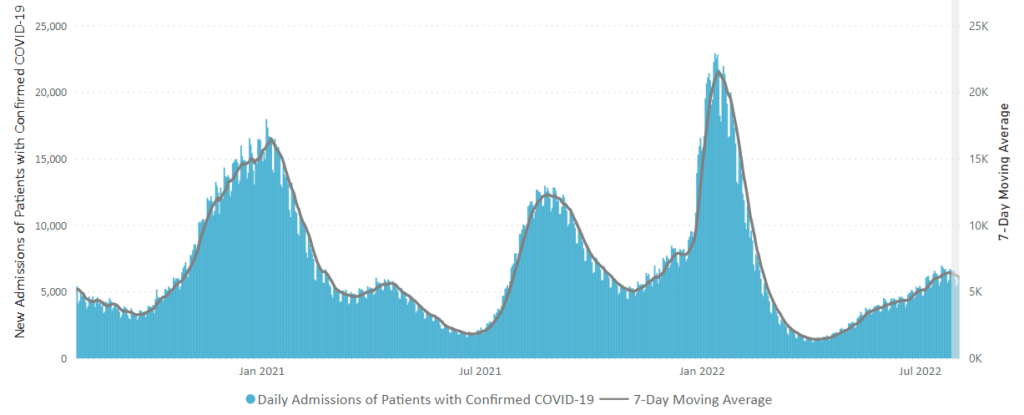
Here’s the CDC’s Daily Trends in Number of New COVID-19 Hospital Admission chart from its weekly review.
The CDC’s weekly review adds, “The current 7-day daily average for August 3–9, 2022, was 6,003. This is a 2.6% decrease from the prior 7-day average (6,163) from July 27–August 2, 2022.”
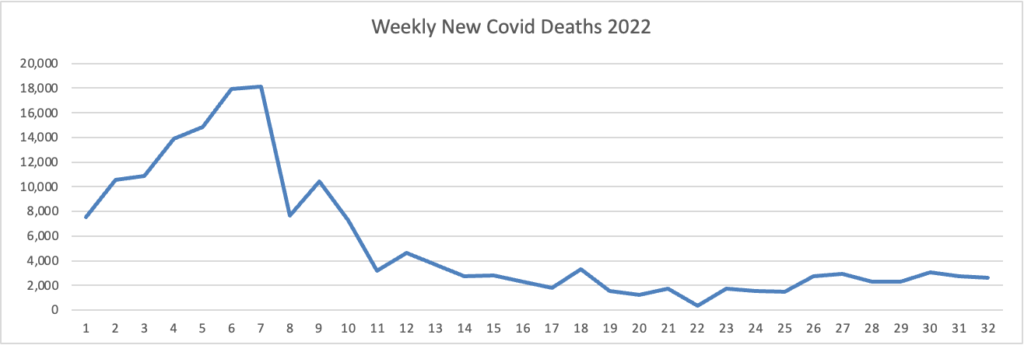
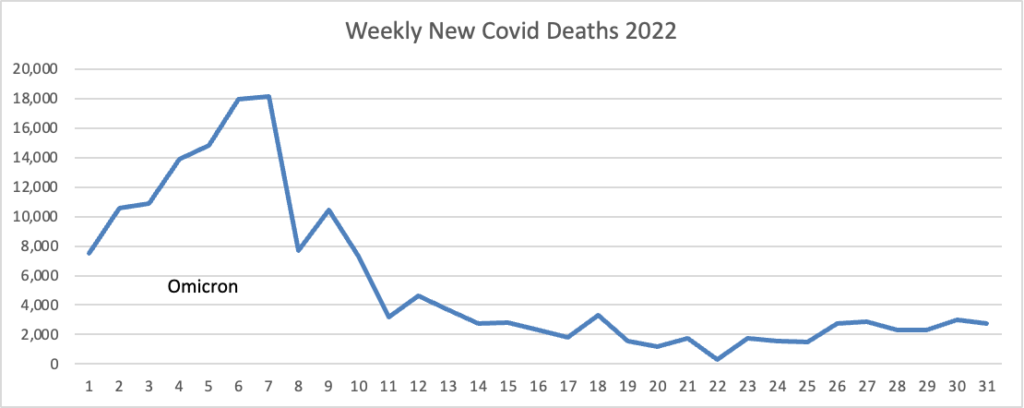
Here’s the FEHBlog latest daily chart of new Covid deaths for 2022:
Unfortunately, both labels fell off this chart. The missing label under the horizontal axis 3 -5 reads Omicron, and the missing label over weeks 14 – 17 reads Omicron’s siblings. The CDC’s weekly review adds, “The current 7-day moving average of new deaths (400) has decreased 6.7% compared with the previous 7-day moving average (429).”
New cases, new admissions and new deaths have plateaued and are trending down.
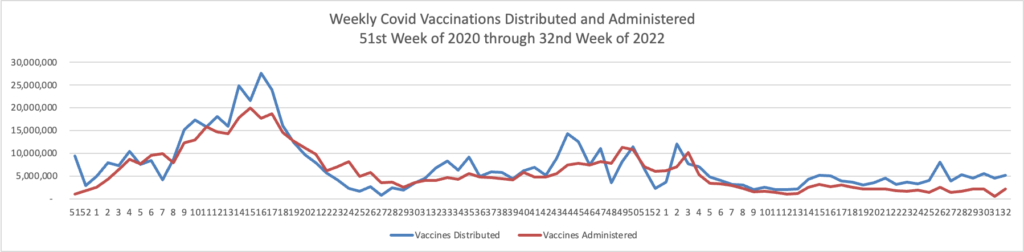
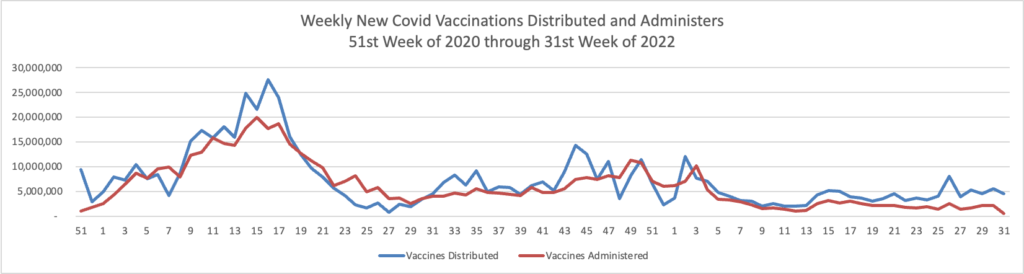
Here’s the FEHBlog’s weekly chart of Covid vaccinations distributed and administered from the first week of the Covid vaccination era in December 2020 to this week.
Administered vaccines jumped back up to over 2 million this week. The CDC’s weekly review adds.
Overall, about 262.0 million people, or 78.9% of the total U.S. population, have received at least one dose of vaccine. About 223.5 million people, or 67.3% of the total U.S. population, have been fully vaccinated.* Of those fully vaccinated, about 107.9 million people have received a booster dose,** but 50.0% of the total booster-eligible population has not yet received a booster dose.
COVID-19 mRNA vaccines have been safe for pregnant women, according to observational data from a large Canadian study.
In fact, the pregnant women reported fewer serious health events than non-pregnant women in the 7 days following vaccination and a similar number of events as a control group of unvaccinated pregnant respondents, as researchers led by Manish Sadarangani, DPhil, of the BC Children’s Hospital Research Institute in Vancouver, reported in The Lancet Infectious Diseases.
The Wall Street Journal reflects on yesterday’s CDC easing Covid restrictions intended to shut down the disease, a state which will not happen anytime soon.
Federal health officials’ move this week to relax pandemic precautions gave business leaders the momentum many have been looking for to return to pre-Covid behaviors.
The new guidelines, issued Thursday by the Centers for Disease Control and Prevention, generally bring the federal guidance in line with policies that had already shifted at companies, schools and public transportation, among other settings. The agency said it no longer recommends that people quarantine after being exposed to the virus, as long as they don’t feel sick, get tested after five days and wear a high-quality mask around others for 10 days.
Many executives and city leaders who had been struggling to break pandemic work-from-home habits see this as a boost to their halting efforts to bring people back into the workplace. They say that previous CDC recommendations made it difficult to enforce their policies, since one exposure could send an entire team home.
It’s worth noting that the CDC issued the revised guidance even though its Spring 2022 innovation based on community levels of the Covid is blinking red.
Overall, 51 out of 52 jurisdictions* had high- or medium-level counties this week. Nevada is the only jurisdiction to have all counties at low Community Levels.
The American Hospital Association calls our attention to another aspect of the Administration’s revised guidance:
The Food and Drug Administration yesterday advised people who get a negative result from an at-home COVID-19 antigen test to test themselves again after 48 hours to reduce the risk of missing an infection and spreading the virus to others.
“Today’s recommendations are based on the latest study results from people with likely omicron infection showing that repeat testing after a negative at-home COVID-19 antigen test result increases the chance of an accurate result,” the agency said
Govexec brings us up to date on the ongoing litigation against the federal government’s Covid vaccination mandate
Remember the vaccine mandate for federal contractors that President Biden issued last September?
Ambika Biggs, a partner at the law firm Hirschler who specializes in government contracting, told Government Executive earlier this week the matter is likely to be appealed to the Supreme Court, especially if there is a circuit split on decisions.
These cases really “come down to the interpretation of the Federal Property and Administrative Services Act, which is just called the Procurement Act” and “whether President Biden had authority under that act to issue the executive order that put the federal contractor mandate in place,” said Biggs. The main argument she’s seen in the pleadings is that “there wasn’t a close enough nexus between wanting an economical and efficient system for procurement and the actual vaccine mandate,” and the mandate was more about public health, which is usually under states’ jurisdiction.
The FEHBlog does not expect this issue to get to the Supreme Court.
From the monkeypox front, Beckers Payer Issues recounts seven payer reactions to the announcement of a public health emergency.
From Capitol Hill, the American Hospital Administration reports
The House today voted 220-207 [along party lines] to pass the Senate’s [budget reconciliation bill] (H.R. 5376), sending it to President Biden for his signature. Passed by the Senate Sunday, the roughly $700 billion social spending package would extend for three years the American Rescue Plan Act’s expanded subsidies for coverage purchased through the Health Insurance Marketplaces; allow Medicare to negotiate prices for insulin and certain other drugs; implement tax changes and spending subsidies to address climate change; and reduce the deficit, among other provisions.
The International Foundation of Employee Benefit Plans offers six aspects of the legislation that are relevant to employers and health plan sponsors.
While the prescription drug provisions of the law are tied only to Medicare Parts B and D, employers and plan sponsors that provide retiree health care benefits, especially through employer group waiver plans (EGWPs), will want to be familiar with this legislation and its impact. They may wish to discuss changes with their advisors to see how their plans may be affected.
That’s good advice.
From the U.S. healthcare costs front, the benefits consulting firm Mercer announced
While significantly higher than the increase of 4.4% projected for 2022, the 2023 increase lags overall inflation, which is currently running at about 9% (see Figure 1). According to Sunit Patel, Mercer’s Chief Actuary for Health and Benefits, “Because health plans typically have multi-year contracts with health care providers, we haven’t felt the full effect of price inflation in health plan cost increases yet. Rather it will be phased in over the next few years as contracts come up for renewal and providers negotiate higher reimbursement levels. Employers have a small window to get out in front of sharper increases coming in 2024 from the cumulative effect of current inflationary pressures.”
From the U.S. healthcare business front, Becker’s Payer Issues reports
Humana has completed the sale of a 60 percent stake in its subsidiary Kindred at Home’s hospice and personal care business to the private equity firm Clayton, Dubilier & Rice. The divisions have been restructured into a standalone company, according to an Aug. 11 Humana news release. The $2.8 billion deal was first announced in April. “Humana will continue to support the long-term success of these operations through our minority ownership and ongoing strategic partnership,” CFO Susan Diamond said in the news release.
Health Care Service Corp. has signed an agreement to purchase Trustmark Health Benefits from employee benefits firm Trustmark for an undisclosed amount. HCSC, the parent company of BCBS Illinois, Montana, New Mexico, Oklahoma and Texas, said in an Aug. 11 news release the acquisition would allow the company to serve more members that desire more customizable health benefits. Trustmark Health Benefits provides voluntary benefits, fitness management products and small group plan administration. The Lake Forest, Ill.-based company said no changes to benefits for existing members will occur when the deal is expected to close later this year.
UnitedHealthcare is rebranding one of its fastest-growing health plan designs. Surest plans, first launched in 2016 as Bind, are available nationwide for self-funded employers and in 11 states for fully insured plans. UHC said it plans to make Surest available as an option for fully insured customers in five more states by the end of the year. Surest plans have the fastest growth rate among its employer-sponsored plan designs, the insurance giant said Thursday.
From the Capitol Hill front, Health Affairs Forefront offers articles from
Prof. Katie Keith on the Affordable Care Act provisions in the budget reconciliation bill (H.R. 5376) that the House of Representatives will take up on Friday, and
Prof. Rachel Sachs on the Democrats’ drug pricing proposal in that bill.
The FEHBlog found information in Prof. Sachs’ article about the proposed $35 cap on insulin copayments.
[T]he IRA was drafted to include a $35 out-of-pocket cap on insulin not only for Medicare beneficiaries, but also for privately insured patients. The parliamentarian ruled that the application of this out-of-pocket cap to privately insured patients did not comply with the reconciliation rules. Rather than unilaterally remove this provision (as the Democrats did with the inflationary rebate provision), Democrats chose to advance the bill with the provision included. Republican Senators then chose to challenge its inclusion, and 43 Republicans voted to strip the $35 out-of-pocket cap for privately insured patients from the bill, enough to result in its removal. (Although seven Republicans voted with all 50 Democrats to keep the cap, the provision needed 60 votes to remain in the bill.)
The Hill adds “Senate Majority Leader Charles Schumer (D-N.Y.) said Monday night that he is going to bring a $35 cap on [non-Medicare] patients’ insulin costs back up for a vote this fall after Republicans blocked it over the weekend.”
Roll Call discusses the cost shifting between Medicare and other insurance programs, including the FEHBP, once the law is enacted and takes effect. Medicare does not negotiate prices with providers; it sets them.
President Biden announced on Wednesday his intent to appoint a prominentsurgeon and professor who has been at the vanguard of advances in cancer treatment to lead the federal government’s main agency for cancer research and training.
The president will appoint Dr. Monica Bertagnolli to be director of the National Cancer Institute, part of the National Institutes of Health, which has about 4,300 employees and had a $6.35 billion budget in fiscal 2021. She is currently the Richard E. Wilson professor of surgery in the field of surgical oncology at Harvard Medical School, a surgeon at Brigham and Women’s Hospital, and a member of the Gastrointestinal Cancer and Sarcoma Disease Centers at Dana-Farber Cancer Institute, a top cancer hospital. Bertagnolli will be the first woman to hold this position.
“Throughout her career, Dr. Bertagnolli has been at the forefront of the field of clinical oncology, advancing, in particular, current understanding of the gene that promotes gastrointestinal cancer development,” said an announcement from the White House. “As a physician-scientist, she led gastrointestinal science initiatives from 1994 to 2011 within the [National Cancer Institute]-funded Cancer Cooperative Groups.” She also served as the chief of the division of Surgical Oncology for the Dana-Farber Brigham Cancer Center from 2007 to 2018.
Good luck, Dr. Bertagnolli.
From the omicron and siblings front, Forbes reports
Pfizer and BioNTech have completed clinical trials for vaccines that include specific protection against the original omicron variant. Now the two companies have begun testing for vaccines specific to the BA.4 and BA.5 Omicron subvariants, which are the fastest spreading variants of Covid-19 in the United States. Manufacturing for the new vaccines has already begun, and could be rolled out as early as October pending regulatory approvals. That’s good news as we approach the fall and winter, which have been the times of year where Covid spread is at its highest. Competitor Moderna has also begun testing an omicron-specific booster, but the FDA has not yet authorized any Omicron-specific vaccines.
Researchers have identified monkey antibodies that are effective against numerous Covid variants and other coronaviruses, a discovery that could help scientists develop better vaccines and prepare for future pandemics as pharma firms race to update their shots.
If the monkey antibodies research is successful, then the WHO definitely should change monkeypox’s name.
From the medical research front, STAT News tells us
With the tumultuous rollout of Aduhelm behind them, partners Biogen and Eisai have the rare opportunity for a do-over, with all-important data on their next Alzheimer’s disease therapy expected next month.
By the end of September, the world will learn whether lecanemab, another treatment aimed at toxic brain plaques called amyloid, can significantly slow the cognitive decline that characterizes Alzheimer’s.
The outcome is vitally important for millions of patients awaiting a medicine that can meaningfully impact the disease, and success could spell a massive financial windfall for Biogen and Eisai. Failure would damage — though not destroy — the idea that targeting amyloid might ever make for an efficacious treatment.
Fingers crossed for a successful outcome.
From the U.S. healthcare business front, Fierce Healthcare reports
Amazon Care, which currently offers virtual health visits, in-person primary care visits at patients’ homes or offices and prescription delivery, is adding behavioral health care to its slate of services.
Amazon’s health service business plans to team up with teletherapy startup Ginger as an optional add-on to Amazon Care. Through the partnership, Amazon Care users will be connected to Ginger’s on-demand mental health services including behavioral health coaches, licensed therapists and psychiatrists, according to a live website about the service. * * *
The new service hasn’t launched yet, according to people familiar with the matter, Business Insider reported.
As an aside, Smart Brief discusses telemedicine in pediatrics.
Fierce Health also tells us
A company with a long history of providing medical supplies for chronic conditions is expanding its business into monitoring and coaching services for diabetes patients.
CCS, which now includes CCS Medical and CCS Health, aims to provide a more integrated experience for chronic care management, Tony Vahedian, CEO of CCS, said in an interview. * * *
“We believe we’re in the appropriate position to really take that fragmented experience and make it an integrated, seamless experience because not only can we deliver the products at the time, but we also can coach them and provide that clinical care,” the CEO noted. CCS can combine its home-delivered medical supplies business with accredited clinicians supported by proprietary data and technology to simplify the patient experience, he added.
The company supports more than 200,000 patients living with chronic conditions in the U.S. and delivers more than 1.2 million shipments of medical supplies to patients in their own homes.
From the nudging front, Health Payer Intelligence shares another survey illustrating that participants in employer-sponsored health plans need more help with health plan literacy.
The Federal Times seeks to project the timeline for implementing the new law requiring the Veterans’ Administration to cover illnesses contracted by Iraq and Afghanistan veterans who were exposed to burn pit smoke while overseas.
The Republicans on the House Ways and Means Committee offer their perspective on the budget reconciliation bill that Senate passed yesterday and the House will take up this Friday.
From the OPM front, the FEHBlog noticed today that its Office of Inspector General (OIG) has posted on its revamped website the OIG’s semi-annual report to Congress for the period ended March 31, 2022. This report is always worth a gander to those who are interested in the FEHB Program.
From the Omicron and siblings front, the Wall Street Journal reports
Parents are having their say about the Covid-19 vaccines for children under 5, and for most, the answer so far is no.
More than a month after the U.S. Centers for Disease Control and Prevention recommended shots for about 17.4 million childrenages 6 months through 4 years, about 4% to 5% of them have received a shot, according to the most recent agency data and population estimates from the American Academy of Pediatrics.
By contrast, the vaccination rate for children 5 to 11 years reached about 18% a month after the CDC first recommended shots last November. The rate now stands at about 38%. * * *
Uptake has varied by state, recent counts from around the U.S. show. In Massachusetts, roughly 40,541 children under 5, about 11% of the state’s population in that age group, have received one dose. In New Jersey, more than 21,000 young children, or 4.6% of the children under 5 in that state, have received one dose.
A lawyer writing on the Society for Human Resource Management advises “employers with workers who test positive for COVID-19 should follow guidance from the Centers for Disease Control and Prevention (CDC), including its guidelines on quarantining and isolation, to minimize safety and legal risks, even though the guidance is somewhat complex.”
From the public health front, the Department of Health and Human Services announced today its Health Resources and Services Administration (HRSA) is
awarding nearly $90 million in American Rescue Plan funding to nearly 1,400 community health centers across the country to advance health equity through better data collection and reporting. On Friday, August 5, President Biden issued a proclamation on National Health Center Week to recognize the vital role health centers play in safeguarding the well-being of Americans and honor the heroic staff who keep these facilities running.
What’s more, the American Hospital Association tells us
[HRSA] today awarded $45.7 million from the American Rescue Plan Act [ARPA]to develop the public health workforce in rural and tribal communities. The grants will help train dental hygienists, medical and dental assistants, doulas and other community health workers; health information technology and telehealth technical support staff; community paramedical workers; and respiratory therapists and care coordinators for patients with long-term COVID-19 effects and chronic medical conditions.
In addition to the ARPA grants, the agency awarded $9.7 million to help hospitals and others establish new medical residency programs in rural communities; $2.9 million to improve health outcomes in rural counties; and nearly $1 million to improve access to care for rural veterans.
From the No Surprises Act front, Healthcare Dive informs us
The Medical Group Management Association, which represents physician practices, is urging the HHS and the CMS to delay enforcing certain requirements of the No Surprises Act to allow providers time to understand and implement the mandates.
In a letter to HHS Secretary Xavier Becerra and CMS Administrator Chiquita Brooks La-Sure, MGMA asked that medical group practices be given six months’ notice before enforcement of additional surprise billing requirements.
The provider group requested the enforcement delay following publication of more anticipated rulemaking including an advanced explanation of benefits, continuity of care protections and provider directory requirements.
The FEHBlog supports the MGMA’s position because Congress goofed in the NSA by not treating the good faith estimate and advance EOB as HIPAA electronic transaction standards.
STAT News discusses the stress that providers and payers are experiencing as they wait for the Labor Department to issue its final rule (following receipt of public comments on its interim final rule) about the NSA’s independent dispute resolution process.
Karuna Therapeutics said Monday that a novel combination pill reduced psychosis and related symptoms experienced by patients with schizophrenia, achieving the main goals of a late-stage clinical trial.
With positive study results in hand, the Boston-based biotech intends to submit a marketing application with the Food and Drug Administration by the middle of next year. If approved, the Karuna drug would usher in the first new class of medicines for the treatment of schizophrenia in decades.
Called KarXT, the Karuna drug targets muscarinic acetylcholine receptors in the brain to reduce psychotic symptoms. Current antipsychotics — which mostly block dopamine receptors — have become blockbuster schizophrenia medicines despite causing troubling side effects like weight gain and somnolence. Peak sales for KarXT could also reach into the billions of dollars, analysts forecast.
Kaiser Permanente posted a thinned operating margin and nearly $1.3 billion net loss during its second quarter “driven largely by investment market conditions,” according to topline financials for the quarter ended June 30 reported Friday evening.
The massive integrated nonprofit health system notched $23.47 billion in total operating revenues, representing a minor 0.9% dip from the second quarter of last year. Total operating expenses inched nearly 0.2% upward year over year, to $23.38 billion.
The result was an operating income of $89 million (0.4% operating margin) during the most recent quarter, down from the prior year’s $349 million (1.5% operating margin).
“Much like the entire health care industry, we continue to address deferred care while navigating COVID-19 surges and associated expenses. Kaiser Permanente’s integrated model of providing both care and coverage enables us to meet these challenges as demonstrated by our moderate increase in year-over-year operating expenses for the second quarter,” EVP and Chief Financial Officer Kathy Lancaster said in a statement accompanying the filing.
Pfizer on Monday said it has agreed to acquire Global Blood Therapeutics for $5.4 billion in a deal that will hand it a recently approved drug for sickle cell disease, as well as two other experimental medicines for the rare blood condition. Under terms of the deal, Pfizer will pay $68.50 in cash per Global Blood share * * *. * * * Pfizer and Global Blood expect the deal, which has been approved by the boards of directors at both companies, to close as early as the fourth quarter, pending the sign off regulators and Global Blood shareholders.
Becker’s Hospital Review is running a series on health information interoperability:
Health data interoperability has long been a goal of health IT executives and policy experts. But it’s 2022 — and the healthcare system doesn’t appear all that close to getting there.
Becker’s spoke to experts from health systems, industry and academia on what it will take to create an open exchange of healthcare information in the U.S.
The first entry in the series is a Q&A with Donna Roach, CIO of University of Utah Health in Salt Lake City
The Senate passed its budget reconciliation bill (H.R. 5376) this afternoon by a 51-50 vote, with Vice President Harris casting the deciding vote. The Senate Democrats have created a one-page summary of the bill.
The deal would dedicate $64 billion to extending for three years the Affordable Care Act subsidies that first kicked in under the 2021 American Rescue Plan. Nearly all of the 13 million people who get federal subsidies under the ACA would be spared from higher health-insurance premiums they would see next year without an extension. * * * The change would push the next expiration beyond the 2024 election.
The measure would also allow Medicare to negotiate the cost of some prescription drugs with pharmaceutical companies, a longtime goal of many Democrats that has been opposed by the drug industry, which says it would stifle innovation. That move would save the government $288 billion, according to the summary.
Here is a link to the Senate Democrat’s summary of the Medicare changes.
[While Medicare was cleared [yesterday] to negotiate drug prices for the first time by the Senate’s top rules official, the Democrats’ proposal intended to cap price increases for prescription drugs in the commercial market was blocked. * * *
The rulings are a partial victory for drug makers, who could try to make up their lost profits in Medicare on private insurers.
Axios notes that during the amendment “vote-a-rama” preceding the vote on H.R. 5376, a provision to cap insulin copayments at $35 was stripped from H.R. 5376.
The House of Representatives will convene on Friday, August 12, to consider and, in all likelihood, pass H.R. 5376. Otherwise, both Houses of Congress are now on their August State/District work break.
In U.S. healthcare business news, the Wall Street Journal reports
CVS Health Corp. is seeking to buy Signify Health Inc., according to people familiar with the matter, as the drugstore and insurance giant looks to expand in home-health services.
Signify Health is exploring strategic alternatives including a sale, The Wall Street Journal reported this past week. Initial bids are due this coming week and CVS is planning to enter one, some of the people said. Others also are in the mix, they said, and CVS could face competition from other managed-care providers and private-equity firms.
There is no guarantee any of them will reach a deal for Signify, which has a market value of around $4.7 billion after its shares rose on the news of a potential sale.
From the Rx coverage front, BioPharma Dive informs us
A new targeted treatment for breast cancer could reshape how doctors classify and treat the disease, offering another option for people whose tumors have spread or are unable to be removed through surgery.
On Friday, the Food and Drug Administration approved Enhertu, a medicine developed by AstraZeneca and Japanese drugmaker Daiichi Sankyo, for patients with advanced breast cancer that has low levels of a protein called HER2. It’s the first targeted drug to be approved for this group of patients.
For more than two decades, HER2 status has shaped treatment of breast cancer. Named after the gene that encodes it, the protein’s presence in high levels is linked to more aggressive tumors that grow and spread faster. But the approval in 1998 of a HER2-targeting drug called Herceptin gave doctors a powerful treatment to combat breast cancers positive for the protein. Since then, several other drugs aimed at HER2 have joined Herceptin on the market.
Until now, HER2 status has been black or white — either positive or negative. However, testing showed Enhertu to be dramatically effective in treating tumors with very low levels of HER2, levels that would typically be considered negative.
The drug’s approval therefore creates a new classification on which doctors can act. About 60% of breast cancer patients who would previously be categorized as having HER2-negative tumors can be now be counted as HER2-low and potentially receive Enhertu, the FDA estimated. HER2-negative cancers are estimated to be by far the most common, accounting for between 80% to 85% of the more than 250,000 people who are diagnosed with breast cancer in the U.S. each year.
From the health information technology front, the FEHBlog picked up this tidbit from a Health Data Management email from “Fred Bazzoli, Editor-in-Chief” this morning:
Much has been changing in healthcare– for providers, payers and consumers.
With a lot of change to assimilate, it’s no wonder that the results are delayed and hard to see. A case in point is healthcare APIs that enable patients to access their medical data. Industry players spent heavily to ready systems for patients to use APIs to access their records. But at this week’s WEDI Summer Forum in Chicago, attendees reported that there was little or no activity in patients using such capabilities. Shoot, only 5 percent to 20 percent of patients are using portals for that purpose now, one payer executive at the forum estimated – so it will take time for them to learn about these apps and get used to using them. Consumers don’t want multiple sources of medical information, or services…they want simplicity, which change doesn’t always seem to provide immediately.
Change is also hard – WEDI is compiling challenges with rules requiring providers to provide patients with good faith estimates. Seemingly simple, providing accurate estimates is wrought with difficulty and peril, as forum attendees heard (see my story next week). More time is needed, WEDI contends.
Slowing down change to allow for consumer adjustment seems to be the right course of action now.
From the public health front, the American Medical Association shares what doctors wish their patients knew about family immunizations.
Based on the CDC’s Covid Data Tracker and using Thursday as the first day of the week, here is the FEHBlog’s latest weekly chart of new Covid cases:
The CDC’s weekly review of its Covid statistics indicates
As of August 3, 2022, the current 7-day moving average of daily new cases (117,351) decreased 7.3% compared with the previous 7-day moving average (126,537).
CDC Nowcast projections* for the week ending July 30, 2022, estimate that the combined national proportion of lineages designated as Omicron will continue to be 100% with the predominant Omicron lineage being BA.5, projected at 85.5% (95% PI 83.8-87.0%).
Here’s the CDC’s chart of “Daily Trends in Number of New COVID-19 Hospital Admissions in the United States”:
The CDC’s weekly review notes “The current 7-day daily average for July 27–August 2, 2022, was 6,112. This is a 4.4% decrease from the prior 7-day average (6,396) from July 20–26, 2022.”
U.S. hospitalization data indicate the latest Covid-19 surge is starting to cool, marking a hopeful sign after months of sustained, high virus transmission due to BA.5 and other Omicron subvariants.
The seven-day average for people hospitalized with Covid-19 has recently flattened, while numbers of newly admitted patients have mostly trended lower since late July, federal data show. Though Covid-19 cases are loosely tracked now, as people test more at home, hospital data can reflect how much the virus is spreading in communities.
“We definitely have hit the plateau,” said Eric Topol, director of the Scripps Research Translational Institute in La Jolla, Calif.
The news is welcome, he said, as the U.S. nears the weeks in which most children will be crowding back into schools. Colleges are scaling back Covid-19 precautions for the fall as they prepare for an influx of students on campus.
Here’s the FEHBlog’s latest weekly chart of new Covid deaths:
The CDC’s weekly review states “The current 7-day moving average of new deaths (378) has decreased 4.9% compared with the previous 7-day moving average (397).” The Wall Street Journal adds
The U.S. has recently averaged 377 reported Covid-19 deaths a day, the CDC data show, far below all-time highs but above the low hit last summer. Known cases recently averaged about 117,000 a day, down slightly over the past week, though epidemiologists believe the true number of infections is significantly higher.
Here’s the FEHBlog’s weekly chart of Covid vaccinations distributed and administered from the beginning of the Covid vaccination era, the 51st week of 2020, through the 31st week of this year.
Covid vaccines administered dropped to around 500,000 last, a new low.
The Wall Street Journal reports
As of Thursday there were 1,344 counties—about 42% of the total—that have high Covid-19 community levels based on case and hospitalization trends, according to the Centers for Disease Control and Prevention. This is down 133 counties from the CDC’s count a week earlier.
About 55% of the U.S. population is now in a high-ranked county with elevated levels of disease, still significantly up from levels below 1% in March and April, but down from 61% a week earlier.
In sum, things are looking up from a Covid era perspective.
From the monkeypox front, the CDC released an information sheet on Monkeypox and Safer Sex.
From the patient safety front, Cardiovascular Business informs us
In 1999, the Institute of Medicine published a shocking report on medical errors that led to in-hospital deaths, noting that as many as 98,000 people per year were dying due to preventable errors.
Now, more than two decades later, are things any better? A team of researchers explored that very questions in JAMA, drawing mostly optimistic conclusions.[1]
To determine whether adverse in-hospital events are on the decline, Noel Eldridge, MS, of the U.S. Department of Health and Human Services, and coauthors looked at data from the Medicare Patient Safety Monitoring System from the years 2010 and 2019. The total number of adverse events dropped from 218 to 139 adverse events per 1,000 discharges for acute myocardial infarction (AMI), and from 168 to 116 adverse events per 1,000 discharges for heart failure, suggesting a significant improvement over time.
The Senate is “on track” to start debating a roughly $300 billion deficit-reducing budget package Saturday after Democrats reached agreement late Thursday on changes to the bill needed to secure 50 votes, Senate Majority Leader Charles E. Schumer said.
The changes, the New York Democrat said at a news conference Friday, include dropping a provision modifying the taxation of “carried interest,” providing exemptions to the 15 percent corporate minimum tax that would reduce its estimated revenue raised over 10 years from $313 billion to $258 billion, and adding some climate provisions related to drought.
“We’re feeling pretty good,” Schumer said, noting he believes the agreement will have the votes to pass.
If so, the bill would then go to the House, which is expected to reconvene Aug. 12 to vote on it, according to a notice Friday from Majority Leader Steny H. Hoyer, D-Md.
Fierce Health summarizes the second quarter results of publicly traded health insurers.
A STATS News journalist provides three takeaways from the this year’s Alzheimer’s Association International Conference, which he attended.
The Senate is expected to begin consideration of Democrats’ climate, tax and health care package on Saturday, leaving about two days for the party to shore up support for the bill.
Senate Majority Leader Charles E. Schumer said Thursday that he’s expecting a vote on the motion to proceed Saturday afternoon, which would follow a nomination vote he scheduled for 12:30 p.m.
The motion to proceed is a simple majority threshold; no Republicans are expected to back it.
If Democrats can secure the votes to move forward, it would trigger up to 20 hours of debate before a “vote-a-rama,” when senators can offer unlimited amendments and motions to delay the process. The debate time is equally divided between the parties and senators on either side can choose to yield back time in order to get to the vote-a-rama quicker.
It remained unclear Thursday afternoon whether party leaders had secured crucial backing from Sen. Kyrsten Sinema. * * *
Democrats are also working to wrap up the “Byrd bath,” in which the Senate parliamentarian hears arguments from both parties and issues opinions on whether provisions meet conditions of the budget reconciliation rules. Reconciliation allows the bill to avoid a filibuster and pass with only Democrats’ votes in the 50-50 Senate. * * * [Sen.] Sinema is expected to wait for the process to play out before making her position on the package known.
While the FEHBlog was writing this post, Politico reports
Sen. Kyrsten Sinema announced on Thursday night that she’s signed off on Democrats’ climate, tax and health care legislation after securing a handful of changes.
The Arizona Democrat was not consulted during July’s dealmaking between Senate Majority Leader Chuck Schumer and Sen. Joe Manchin, but after changes to several tax provisions she okayed the agreement on Thursday. “We have agreed to remove the carried interest tax provision, protect advanced manufacturing, and boost our clean energy economy in the Senate’s budget reconciliation legislation. Subject to the Parliamentarian’s review, I’ll move forward,” Sinema said.
From the Omicron and siblings front
The New York Times explores the question “Is This What Endemicity Looks Like?” The article points out “The basic footprint of the disease has been consistent for a few months.”
We’ve been at roughly the same number of hospitalizations and deaths in the country since the end of the initial Omicron wave in the winter. And because so much of that has to do with how much better our immune systems are working against Covid than in the past, there’s probably no reason to think that those dynamics are going to dramatically change unless there’s an out-of-left-field new variant like the original Omicron.
And I think that fits the layperson’s understanding of what an endemic disease is: It’s circulating, but it’s sort of in the background, and while there are some little peaks and some little valleys, they aren’t so dramatic that they threaten to really upend life at a community level, let alone at a national level. That’s a pretty fair description of where we are right now.
While Omicron remains a dangerous virus, particularly for the elderly, which of course is where we started, we now have vaccines against severe illness and treatments for the virus.
Most patients with smell or taste dysfunction related to COVID-19 reported complete recovery of their senses at 2 years, according to a cross-sectional survey conducted in Italy.
Among 119 patients with smell or taste dysfunction within 4 weeks of COVID onset, 88.2% reported complete resolution at 2 years, 9.2% reported a decline in symptom severity, and 2.5% reported unchanged or worsening symptoms, said Paolo Boscolo-Rizzo, MD, of the University of Trieste, and colleagues.
And Los Angeles schools plan on updating COVID-19 protocols for the upcoming school year by dropping “overly aggressive” testing, masking, and vaccination requirements. (KTLA).
The White House today declared monkeypox a public health emergency.
“We are prepared to take our response to the next level in addressing this virus and we urge every American to take monkeypox seriously,” Health and Human Services Secretary Xavier Becerra said to reporters during a briefing on Thursday.
A public health emergency can trigger grant funding and open up more resources for various aspects of a federal response. It also allows the Secretary to enter into contracts for treatments and other necessary medical supplies and equipment, as well as support emergency hospital services, among other things. Public health emergencies last for 90 days but can be extended by the Secretary.
CDC Director Rochelle Walensky, said the declaration will provide resources and increase access to care. She also said it will expand the CDC’s ability to share data.
Also Thursday, FDA Commissioner Robert Califf announced the agency was considering allowing Bavarian Nordic’s Jynneos, the only vaccine licensed in the United States to prevent monkeypox, to be given in two doses that are one-fifth the size of the licensed doses, via intradermal administration. Doing so could allow five times as many people to be vaccinated with existing supplies than if the licensed dosage was employed.
The vaccine is licensed as a two-dose product, with the doses administered via intramuscular injection 28 days apart.
“We believe this could be a promising approach,” Califf said.
In other public health news, the Department of Health and Human Services announced
Our nation’s blood and plasma supply dropped to historic lows during the COVID-19 pandemic. While some areas of the country have seen improvement, other areas are still struggling to meet the demand. Blood and plasma are needed on an ongoing basis to treat a variety of life-threatening conditions, which is why the U.S. Department of Health and Human Services (HHS), is launching a new campaign, Giving = Living. * * *
Visit hhs.gov/givingequalsliving to learn more about the importance of donation and make an appointment at a donation location near you.
Cigna reported net income increased 6% year over year to $1.6 billion during the second quarter as fewer people were admitted to the hospital, had fewer surgeries and visited the emergency room less.
The Connecticut-based insurer said medical costs for both COVID-19 and non-COVID-19 care were lower than projected. The insurer’s medical loss ratio, an important measure of how much is spent on medical care, fell to 80.7% for the second quarter. Analysts said price hikes helped the MLR, too.
As a result of the quarterly performance, Cigna raised financial targets for the year for revenue and income from operations.
Telehealth company Amwell is working with CVS Health to roll out the retail drugstore giant’s new virtual primary care service.
CVS announced at the end of May plans to launch a virtual care service that gives consumers access to primary care, on-demand care, chronic condition management and mental health services. Eligible Aetna and CVS Caremark members will be able to use the virtual primary care service to access healthcare services on demand, whether at home or in a retail or community-based setting, the drug store company said.
CVS’ virtual care platform is a “consumer-centric offering designed to bring together the many elements of CVS Health ecosystem services into a single integrated experience with a unified digital front door,” Dr. Ido Schoenberg, chairman and co-chief executive officer of Amwell, said during the company’s second-quarter earnings call Thursday.
Elevance Health is betting big on primary care with a new nationwide partnership with Aledade.
The team-up will focus on assisting primary care practices in transitioning to value-based care, to boost health outcomes and lower costs. Independent primary care practices that are within the insurer’s network will be able to access Aledade’s suite of technology and local, in-person services.
Aledade’s platform provides the tools, support and resources that PCPs need to roll out value-based care, the companies said.
Pfizer Inc. will spend $470 million to expand its vaccine research facilities 25 miles northwest of New York City, where the company hopes to maintain its edge in the booming field of messenger RNA, the technology behind its blockbuster Covid-19 shot.
The drugmaker will construct a new building and renovate existing facilities on its campus in Pearl River, New York, which has been the nexus of laboratory research driving its vaccine programs, including the one for Covid in partnership with BioNTech SE.
From the substance use disorder front, NPR explains
Music festivals once frowned upon naloxone, and some banned it. But even though what’s known as harm reduction — the concept of minimizing the negative effects of illicit drug use without trying to stop it altogether — has gained acceptance, it’s far from embraced. Less accepted than naloxone among concert promoters is helping people test their drugs for fentanyl. Companies don’t want to be seen as condoning drug use. They’re also navigating a legal gray area and battling public perceptions. * * *
Overdose deaths continue to climb in the U.S. Drug fatalities topped 100,000nationwide in 2021, with two-thirds caused by synthetic opioids. This has prompted federal and state governmentsto try to think of new ways to combat the crisis, with the Biden administration giving $30 million to support programs that have often operated in the shadows. In the past few years, the Substance Abuse and Mental Health Services Administration also has fully embraced fentanyl test kits.
Still, many communities far beyond music festival grounds are resistant to harm-reduction strategies, especially fentanyl-testing tools. Dr. Yngvild Olsen, director of SAMHSA’s Center for Substance Abuse Treatment, said harm reduction requires an evolution in thinking, and she encourages organizations to consider harm reduction a lifesaving tool — especially when mass overdoses are possible.
From the telehealth front, Health Payer Intelligence reports
Telehealth flexibilities during the coronavirus pandemic contributed to a 26 percent spike in overall utilization of in-network outpatient behavioral health, according to a report from UnitedHealth Group.
“Prior to the COVID pandemic, telehealth was broadly viewed as a potential strategy for improving access to behavioral health care,” the report explained.
“During the pandemic—which saw increased rates of depression, anxiety, and substance use disorder—federal and state policymakers and commercial health plans established temporary flexibilities to increase access to care, and patients and providers increased their use of virtual visits as an alternative to in-person office-based care.”
Democrats may need to make some changes to the tax portion of their budget reconciliation package to earn the support of Arizona Sen. Kyrsten Sinema, including possible removal of a tax increase on investment fund managers and softening a new minimum tax on the biggest corporations.
The bill could also undergo other tweaks as Senate Parliamentarian Elizabeth MacDonough continues her review of the bill. Changes to the prescription drug pricing provisions are already in the works, but many pieces of the package have yet to go through the formal “Byrd bath” to determine whether the language complies with budget rules.
Despite all the work still underway, several Democratic senators said they anticipated voting on the motion to proceed to the reconciliation package as soon as Thursday and beginning the “vote-a-rama” process, in which senators can offer unlimited amendments to the measure, as soon as this weekend.
“As soon as possible, but don’t count on going home on the weekend,” Michigan Sen. Debbie Stabenow, a member of Democratic leadership, said. “We’re probably going to be here all weekend, so get lots of sleep.
The Office of Personnel Management is getting a second in command.
President Joe Biden nominated Rob Shriver to be the OPM deputy director on Aug. 3. * * *
Shriver is a political appointee already, having been the associate director for employee services since January 2021.
If confirmed by the Senate, Shriver would be OPM’s first deputy director since Michael Rigas, who held the job from March 2018 to January 2021, but worked in other administration positions from March 2020 until January 2021.
[Israeli] Hospital workers who got a fourth dose of Pfizer Inc.’s messenger RNA vaccine were far less likely to get Covid than triple-vaccinated peers in a study.
The findings published Tuesday in the American Medical Association’s open access journal are the latest to confirm the benefits of a second booster against breakthrough infections caused by omicron. The study’s authors pointed to an extra dose as a tool to prevent medical staff shortages and spare health systems in times of strain. * * *
Doctors, nurses and other health-care workers who got a fourth mRNA shot in January showed a 7% rate of breakthrough infections. Those with three doses — the third having been administered by the end of September — saw an infection rate of 20%.
The Department of Health and Human Services released two reports on long Covid to support patients and further research.
From the monkeypox front
Beckers Hospital Review explains that the Centers for Disease Control have released isolation guidance “as cases near 6,000.”
The New York Times delves into various aspects of the disease, including what people can do the stay safe.
CVS Health raised its full-year guidance in its second quarter earnings report despite a $77 million decrease in adjusted operating income primarily due to declines in its retail segment.
The company’s Aetna subsidiary boosted earnings with reported gains of 922,000 covered lives compared to the second quarter of last year and growth in all product lines contributing to a nearly 11% rise in revenues year over year.
Adjusted operating income was 9.1% lower in its retail division compared to the year prior due to a decrease in coronavirus vaccinations, “continued pharmacy reimbursement pressure” and the lack of an antitrust legal settlement gain that was recorded in the second quarter last year, according to the earnings report. * * *
In its race to add more primary care services, the executive team further teased acquisition plans, with [CVS Health CEO Karen] Lynch adding that the company could take the “next step on this journey” by the end of this year.
“We can’t be in … primary care without M&A. We’ve been very clear about that,” Lynch said.
[Larry] McGrath [CVS Health senior vice president of business development and investor relations] added that the company has been active in evaluating a wide range of assets around the care delivery space. CVS also signaled that it could potentially pursue multiple acquisitions, adding that there was “no one and done asset” in the market.
Gilead’s cell therapy business outperformed Wall Street expectations during the second quarter. The unit — which currently consists of two products, Yescarta and Tecartus, used to treat various blood cancers — generated $368 million in the three-month period, an increase of 68% year over year, earnings numbers released Tuesday show.
Key to that growth was a recent, first-of-its-kind approval from the Food and Drug Administration. In April, the agency cleared Yescarta as a so-called second line therapy for large B-cell lymphoma that resists or returns within a year of initial treatment with chemoimmunotherapy. Before, Yescarta was used only when patients either relapsed after or hadn’t responded to at least two other kinds of therapies.
CivicaScript’s first product is hitting the market.
The public benefits company and sister to Civica Rx is making its first generic available: 250-mg abiraterone acetate tablets. The drug is used in combination with the steroid medication prednisone as a treatment for prostate cancer that has spread to other parts in the body.
CivicaScript will make the drug available to pharmacies at $160 per bottle of 120 tablets, a typical one-month supply. The company suggests pharmacies sell it to patients at no more than $171 for each bottle. This price is about $3,000 less per month than the average cost for people enrolled in Medicare Part D, which is the largest portion of patients with this type of cancer.
Using CivicaScript’s abiraterone will lead to significant savings for patients both in the deductible phase and in the Part D “donut hole,” where they face the highest out-of-pocket costs, the company said in an announcement (PDF). * * *
“We’re proud the first lower-cost generic drug of our partnership with CivicaScript is entering the market,” said Kim Keck, president and CEO of BCBSA. “This is an important milestone in our shared commitment to help make prescription drugs more affordable for millions of Americans. No one should have to face breaking the bank from buying a life-saving medication.”
From the Affordable Care front, Prof. Katie Keith takes a deep dive into last week’s ACA FAQ 54 on mandated contraceptive coverage under that law.
A survey of nearly 2,500 U.S. healthcare consumers by PYMNTS.com offered more proof that this remains a barrier to consumer trust of the healthcareThe survey revealed that many consumers continue to under budget for their health care –probably because most have little idea about the cost of various procedures and appointments. * * *
For instance, nearly 20% of those surveyed said they “experienced financial distress due to health care costs because they spent more than they could afford in the past 12 months.” A quarter of respondents who said their advance notice cost estimates were accurate said they still spent more than they could really afford. Not surprisingly, 43% of those who received inaccurate cost estimates said they spent more than they could afford. system. PYMNTS.com, a provider of data, news and insights on innovation in payments and the payment-related, conducted the survey to learn how many respondents fell into the unexpectedly high and inaccurate estimate category, and what the outcome for them was in the aftermath. * * *
Regular exercise, regardless of intensity level, appears to slow cognitive decline in sedentary older adults with mild cognitive impairment (MCI), new research from the largest study of its kind suggests.
Topline results from the EXERT trial showed patients with MCI who participated regularly in either aerobic exercise or stretching/balance/range-of-motion exercises maintained stable global cognitive function over 12 months of follow-up — with no differences between the two types of exercise.
“We’re excited about these findings, because these types of exercises that we’re seeing can protect against cognitive decline are accessible to everyone and therefore scalable to the public,” study investigator Laura Baker, PhD, Wake Forest University School of Medicine, Winston-Salem, North Carolina, said at a press briefing.
The topline results were presented at the Alzheimer’s Association International Conference (AAIC) 2022.
More than 3.5 million veterans who were exposed to toxic substances on overseas deployments will gain easier access to health and disability benefits under a bill that cleared the Senate Tuesday.
President Joe Biden is certain to sign the bill into law in the coming days.
The bill would make servicemembers who contracted any of 23 conditions — from brain cancer to hypertension — after being deployed to Iraq, Afghanistan and other combat zones automatically eligible for VA benefits. The measure is expected to cost nearly $280 billion over a decade, according to the Congressional Budget Office.
This law should save the FEHB Program money as the federal workforce has a large cadre of veterans who use veterans’ healthcare. VA facilities charge the FEHB and private sector plans for non-service connected health care. This law confirms that toxic substances treatment to service-connected care for which the VA is liable.
The [VA] bill [also] authorizes leases for 31 new medical facilities at VA to help accommodate the expected surge in patients, which is expected to cost nearly $1 billion. The Congressional Budget Office found the slew of pay and other human resources changes would come with a $5.7 billion price tag over the next decade.
The bill will authorize the department to buy out the contract of health care professionals to recruit them to VA, so long as they make a four-year commitment to the department. VA will have $40 million per year for the buyouts. VA’s health care employees will be eligible for pay boosts worth 50% of their base salaries, up from the current cap of 30%. Overall pay would be capped at level two of the Executive Service pay scale, which is currently $203,000 per year. McDonough has called lifting the pay caps essential for VA’s recruiting and retention efforts and has aggressively pushed Congress to pass the reform.
With regard to the Schumer-Manchin reconciliation bill, the Hill reports that Senators Manchin and Simema are exchanging text on the bill.
From the Omicron and siblings front,
McKinsey and Company offer their assessment of when the Covid pandemic will end.
In this update, we discuss the outlook, the current and potential future use of boosters and therapeutics, and the shifts in response strategies to the COVID-19 crisis around the world. We also introduce the McKinsey COVID-19 Immunity Index—a tool for understanding a community’s current level of risk from the disease.
A group of physicians provides their observations in MedPage Today on how best to investigate the Paxolovid rebound issue.
The debate about “COVID-19 rebound” after nirmatrelvir/ritonavir (Paxlovid) treatment is one of these timely areas warranting further investigation. Continuing down the current path of uncertainty has consequences for how and by whom this antiviral should be used. However, by applying lessons learned from the early days of the pandemic — including acknowledging the importance of randomized controlled trials (RCTs) — we can avoid repeating the same mistakes. To do this, it is necessary to start by defining the question, identifying current knowledge gaps, and only then can one propose scientific solutions to bring a rapid resolution to the COVID-19 rebound controversy.
Paxlovid consists of two drugs: nirmatrelvir, which inhibits a SARS-CoV-2 protease inhibiting viral replication, and ritonavir, which slows the inactivation and breakdown of nirmatrelvir. Per a CDC health advisory released in May, COVID-19 rebound is defined as a return of symptoms or a “new positive viral test after having tested negative” occurring “2 to 8 days after initial recovery.” We just saw this over the weekend in the case of President Biden.
This definition of rebound is challenging and prone to inflating the incidence of rebound. It is possible some individuals identified as having “Paxlovid rebound” may have been experiencing a waxing and waning of COVID-19 symptoms while some unknown number of other reported rebound cases could be due to the known limitations of COVID-19 testing.
Precision Vaccinations tells us that in the near future the federal government will make the Omicron antibody based treatment known as Evusheld available through local pharmacies including “Albertsons, Acme, Jewel-Osco, Pavilions, Randalls, Safeway, Star Market, Vons, CPESN, Amber Specialty Pharmacy, Managed Healthcare Associates, and Thrifty White.”
Hugh Montgomery, Professor of Intensive Care Medicine at University College London, UK, and TACKLE principal investigator, commented in a press release, “Despite the success of vaccines, many individuals such as older adults, individuals with co-morbidities, and those who are immunocompromised, remain at risk for poor outcomes from severe COVID-19.”
“Additional options are needed to prevent disease progression and reduce the burden on healthcare systems, especially with the continued emergence of new variants.”
“The TACKLE (study) results show that one intramuscular dose of Evusheld can prevent these individuals from progressing to severe COVID-19, with earlier treatment leading to even better results.”
From the moneypox front, Fierce Healthcare reports
The White House has named Robert Fenton to serve as the response coordinator for the monkeypox outbreak, as calls for a larger federal role intensify.
Fenton previously helped to coordinate COVID-19 vaccine distribution while working at the Federal Emergency Management Agency. He will work alongside Demetre Daskalakis, M.D., who will be the deputy coordinator.
The coordinators will lead the administration’s efforts on “strategy and operations to combat the current monkeypox outbreak, including equitably increasing the availability of tests, vaccinations and treatments.”
From the Affordable Care Act front, the International Foundation of Employee Benefit Plans informs us
The Internal Revenue Service (IRS) has issued Revenue Procedure 2022-34 providing the indexing adjustment for the required contribution percentage. For plan years beginning in 2023, the required contribution percentage is 9.12%, down from 9.61% in 2022.
The affordability calculation can determine whether an individual can afford employer-sponsored health coverage and affect whether the individual would be eligible for a premium tax credit on the health insurance exchanges. This could affect employers that do not use a safe harbor method to determine whether the coverage they offer is affordable to employees.
For plan years beginning in 2023, employer-provided coverage is considered affordable for an employee if the employee required contribution is no more than 9.12% of that employee’s household income. Because applicable large employers generally do not know their employees’ household incomes, there are three safe harbor methods for calculating affordability.
In the FEHB Program, OPM must assure itself that the lowest premium nationwide FEHB plan premium for the self only option does not cost more than 9.12% of the lowest paygrade federal employee eligible to participate in FEHBP.
From the FEHB front, Fedweek columnist Reg Jones wraps up his series of federal employee and annuitant survivor benefits.
From the Medicare front, Healthcare Dive reports on provider reaction to yesterday’s final CMS rule on Medicare Part A payments to inpatient hospitals beginning October 1, 2022.
Organizations like The American Hospital Association said it was “pleased” by the payment update, a 4.3% bump up from the proposed 3.2%, but added it “still falls short of what hospitals and health systems need to continue to overcome the many challenges that threaten their ability to care for patients and provide essential services for their communities.”
Group purchasing organization Premier agreed, saying the payment update “falls woefully short” of what is needed for health systems. “Coupled with record high inflation, this inadequate payment bump will only exacerbate the intense financial pressure on American hospitals,” SVP of Government Affairs Soumi Saha said in a statement.
Beckers Hospital review offers six takeaways from the final rule.
High operating expenses took their toll on hospitals and physician groups in June, producing negative year-over-year margins for a sixth consecutive month, a new report from Kaufman Hall found. Month-to-month increases in patient volumes were not enough to offset the growing cost of care, the advisory firm said Monday.
Compared with May, operating margins improved, contract labor costs fell as demand slowed, and expenses cooled slightly in the latest month. But the industry has yet to turn the corner on an “enormously difficult year,” the report said.
“Although hospitals are seeing improved volumes and reduced expenses month-over-month, they will likely end up with historically low margins for the remainder of the year,” Kaufman Hall predicted.
Louisiana-based Ochsner Health has officially merged with Rush Health Systems, giving the merged system seven hospitals and more than 30 clinics in the east Mississippi and west Alabama region, according to a Monday release.
New names and branding are being rolled out at regional hospitals under the new brand, Ochsner Rush Health, the release said. Ochsner Rush Health will have 250 staff and contracted physicians and 95 advanced practice providers.
Ochsner Rush Health is also boosting its minimum wage to $12 an hour, impacting more than 400 employees and representing a $1.5 million investment, according to the release.
From the public health front,
Healio offers a bleak outlook for chronic disease in the US over the next forty years “likely stressing an already burdened health care system.”
The Center for Disease Control points to its revamped diabetes website “for people with diabetes or who are at risk for diabetes, and their families and friends.”
From the judicial front,
STAT News tells us
In a significant victory for AbbVie, a U.S. appeals court panel declined to revive a lawsuit that accused the company of using a so-called patent thicket to forestall competition for its Humira medication, a franchise product that generates billions of dollars in sales each year.
The opinion shot down arguments by unions, insurers, and the city of Baltimore, which alleged that AbbVie “abused the patent system” and “erected significant barriers to entry to block biosimilar competition” by filing dozens of patents for the drug. Some of the 132 U.S. patents that the company holds on its medicine extend to 2034, although the basic patent expired in 2016.
The case has been closely tracked over concerns that the use of numerous patents — some of which may offer only marginal improvements or changes to a medicine — are exploited by pharmaceutical companies to protect monopolies at the expense of consumers. This has prompted the Food and Drug Administration and Patent and Trademark Office to jointly examine the issue.
Congress can change the patent system applicable to prescription drugs.
The American Hospital Association reports
The Department of Justice today filed a lawsuit challenging an Idaho law restricting abortion. The complaint seeks a declaratory judgment that the law conflicts with and is preempted by the Emergency Medical Treatment and Labor Act in situations where an abortion is necessary stabilizing treatment for an emergency medical condition. It also seeks an order permanently enjoining the law to the extent it conflicts with EMTALA, which requires hospitals that receive federal Medicare funds to provide necessary stabilizing treatment to patients who arrive at their emergency departments while experiencing a medical emergency.
The FEHBlog hopes that the federal court hearing the case seeks a decision from the Idaho Supreme Court on the scope of Idaho’s abortion law before proceeding with the case. The FEHBlog finds it hard to believe that any U.S. court would interpret its state’s abortion law as overriding obligations created by EMTALA and for that matter the Hippocratic Oath.
Senate Democrats are growing more anxious over maverick Sen. Kyrsten Sinema’s (D-Ariz.) five-day silence on a sweeping proposal to reform the tax code, tackle climate change and reduce the federal deficit.
Democratic lawmakers are privately worried that Sinema’s not happy about being left out of the negotiations between Senate Majority Leader Charles Schumer (D-N.Y.) and centrist Sen. Joe Manchin (D-W.Va.), which resulted in a surprise announcement last week of a major deal.
Govexec.com reports on the Republican response to the Senate Appropriations Committee’s release of its twelve fiscal year 2023 appropriations bills last week.
From the Medicare front, Fierce Healthcare informs us
The Biden administration finalized a 4.3% bump for inpatient payments for the federal fiscal year 2023, an increase compared to the 3.2% that was originally proposed back in April.
The Centers for Medicare and Medicaid Services released on Monday the final Inpatient Prospective Payment System (IPPS) and Long-Term Care Hospital Prospective Payment System rule that updates payments to hospitals. The rule also details health equity quality measures hospitals must now meet for participation in the Inpatient Quality Reporting program.
Here’s a link to the CMS fact sheet on this final rule.
Revcycle Intelligence tells us that last week “CMS released FY23 final rules for hospice providers,inpatient psychiatric facilities, and inpatient rehabilitation facilities. The final rules for fiscal year 2023 include a 3.8% payment increase for hospice providers, 2.5% increase for inpatient psychiatric facilities, and 3.2% boost for inpatient rehabilitation facilities.
Also, last week, CMS released the FY 2023 final rules for skilled nursing facilities. The rule represents a 2.7% payment increase for SNFs.
Fierce Healthcare adds “CMS said Friday [July 29] that it expects the average premium to decrease to $31.50 in 2023, or about 1.8% from the 2022 rate of $32.08.
From the healthcare quality front, the National Committee for Quality Assurance released its Measurement Year 2023 HEDIS and CAHPS guidelines today. NCQA made publicly available a list of adds, drops and other significant changes for MY 2023.
From the U.S. healthcare business front, Bloomberg reports
Labcorp, a diagnostics and laboratory company, is spinning off its clinical trials division into a separate publicly traded company.
Labcorp will house the company’s existing global laboratory business while the new company will manage clinical trials for drug companies. Management said in a release Thursday [July 28] that this structure will allow each division more flexibility to grow within their individual markets.
From the post-Dobbs front, Healthcare Dive tells us
Abortion access nonprofit Just the Pill plans to build a fleet of mobile clinics offering mobile procedural abortion “for the first time in U.S. history,” the nonprofit said. * * *
The group currently operates two mobile clinics in Colorado and plans to build out its network of vans and deploy them in states where abortion is legal but surrounding states have banned the procedure, such as New Mexico, Pennsylvania and Illinois.
“Our mobile clinics will travel to parts of these states based on where the need is greatest,” Julie Amaon, medical director of Just The Pill, told Healthcare Dive. * * *
Mobile health clinics have been held up as an avenue to cut costs and expand healthcare access, especially in underserved or marginalized communities. One 2009 Boston study found that a mobile health clinic, The Family Van, had a return on investment of $36 for every $1 invested in the program. Mobile clinics can also provide primary and preventative care, an important feature given that many regions in the U.S. lack healthcare access.
From the wellness front, Morning Consult provides advice on offering wellness services to younger employees.
While benefits like annual raises and an employee assistance program (EAP) with appointment limits have been alluring, these perks are now expected by many Millennial and Gen Z employees, who will soon make up 75% of the U.S. workforce.
Improving hiring and retention for the shifting workforce starts with understanding the core values that drive younger generations to join, or leave, organizations in the first place – and that’s health and mental well-being, as a whopping 83% of employees place their benefits as a main deciding factor in whether they will stay at their current job.
As a baby boomer, the FEHBlog prefers to refer to the younger crowd as Zoomers over Gen Z.
From the medical research front —
Medscape reports “A simple blood test that looks for a combination of specific RNA snippets may become a novel way to screen for early-onset colorectal cancer, suggests a new study published online in Gastroenterology.”
“The point would be to use this test as a routine part of annual healthcare, or for people in high-risk families every 6 months,” study senior author Ajay Goel, PhD, MS, chair of the Department of Molecular Diagnostics and Experimental Therapeutics at the City of Hope Comprehensive Cancer Center, Duarte, California, told Medscape Medical News.
“It’s affordable, it can be done easily from a small tube of blood, and as long as that test stays negative, you’re good,” Goel said, because even if patients miss a test, the next one, whether it’s 6 months or a year later, will catch any potential cancer.
A study published this week in Nature Communications shows that an automated clinical decision support tool for genetic disease diagnosis and treatment can provide accurate results and disease management guidance within 13.5 hours.
The tool, known as Genome-to-Treatment (GTRx), is a virtual disease management system that integrates whole genome sequencing to provide diagnostics and guidance for 500 diseases, according to a press releasediscussing the study’s findings. The study was completed in collaboration with multiple organizations, vendors, and health systems.
The study states that the 7,200 genetic disorders currently known to medical science result in high levels of morbidity and mortality in children, specifically in neonatal, pediatric, and cardiovascular patients. Approximately 140 million children worldwide suffer from rare genetic diseases, and experts estimate that 30 percent of them will not survive until their 5th birthday.
From the miscellany department, STAT News asks why monkeypox does not have a new name yet. The FEHBlog wonders if monkeypox’s name is changed, then what’s next chickenpox? swine flu?
We use cookies on our website to give you the most relevant experience by remembering your preferences and repeat visits. By clicking “Accept”, you consent to the use of ALL the cookies.
This website uses cookies to improve your experience while you navigate through the website. Out of these, the cookies that are categorized as necessary are stored on your browser as they are essential for the working of basic functionalities of the website. We also use third-party cookies that help us analyze and understand how you use this website. These cookies will be stored in your browser only with your consent. You also have the option to opt-out of these cookies. But opting out of some of these cookies may affect your browsing experience.
Necessary cookies are absolutely essential for the website to function properly. These cookies ensure basic functionalities and security features of the website, anonymously.
Cookie
Duration
Description
cookielawinfo-checbox-analytics
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Analytics".
cookielawinfo-checbox-functional
11 months
The cookie is set by GDPR cookie consent to record the user consent for the cookies in the category "Functional".
cookielawinfo-checbox-others
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Other.
cookielawinfo-checkbox-necessary
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookies is used to store the user consent for the cookies in the category "Necessary".
cookielawinfo-checkbox-performance
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Performance".
viewed_cookie_policy
11 months
The cookie is set by the GDPR Cookie Consent plugin and is used to store whether or not user has consented to the use of cookies. It does not store any personal data.
Functional cookies help to perform certain functionalities like sharing the content of the website on social media platforms, collect feedbacks, and other third-party features.
Performance cookies are used to understand and analyze the key performance indexes of the website which helps in delivering a better user experience for the visitors.
Analytical cookies are used to understand how visitors interact with the website. These cookies help provide information on metrics the number of visitors, bounce rate, traffic source, etc.
Advertisement cookies are used to provide visitors with relevant ads and marketing campaigns. These cookies track visitors across websites and collect information to provide customized ads.