The President released his Administration’s fiscal year 2023 proposed budget today. Here are links to OMB’s budget website and a Roll Call overview of the proposal.
Amend administration of tribal FEHB enrollment system
Expand family member eligibility under FEDVIP (presumably increasing the age limit for eligible children from 22 to 26)
Expand FEDVIP to tribal employees
Expand FEHB to tribal colleges and universities.
OPM also released the agency’s FY 2022 to FY 2026 strategic plan today. Here is a link to OPM’s lookbook on that plan. The lookbook (p. 9) identifies one current agency priority goal related to the FEHBP (out of six in total)
Improve customer experience by making it easier for Federal employees, annuitants, and other eligible persons to make more informed health insurance plan selection. By September 30, 2023, complete user-centered design and develop a minimum viable product for a new, state-of-the-art FEHBP Decision Support Tool that will give eligible individuals the necessary information to compare plan benefits, provider networks, prescription costs, and other health information important to them and their families.
In other government reports, the Centers for Medicare and Medicaid Services issued
the 2021-2030 National Health Expenditure (NHE) report, prepared by the CMS Office of the Actuary, that presents health spending and enrollment projections for the coming decade. The report notably shows that despite the increased demand for patient care in 2021, the growth in national health spending is estimated to have slowed to 4.2%, from 9.7% in 2020, as supplemental funding for public health activity and other federal programs, specifically those associated with the COVID-19 pandemic, declined significantly.
From the Omicron and siblings front —
The Centers for Disease Control posted a new “Quarantine and Isolation Calculator — A tool to help determine how long you need to isolate, quarantine, or take other steps to prevent spreading COVID-19.”
The Institute for Clinicial and Economic Review issued an evidence report on four Covid outpatient treatments, including the Pfizer and Merck Covid pills.
ICER’s evidence ratings for the treatments reviewed include:
Sotrovimab delivers at least a small net health benefit when compared to no active treatment, with the possibility of a substantial net health benefit (“B+”).
[Merck’s] Molnupiravir is at least comparable to no active treatment, with the potential of a small net health benefit (“C+”).
[Pfizer’s] Paxlovid delivers at least a small net health benefit when compared to no active treatment, with the possibility of a substantial net health benefit (“B+”).
Fluvoxamine is at least comparable to no active treatment, with the potential of a small net health benefit (“C+”).
From the health equity front, Health Leaders Media reports
Despite willingness to address social drivers of health, two-thirds of physicians report inadequate time or ability to act, according to a new survey report.
KEY TAKEAWAYS
Nearly all physicians reported that at least one social driver of health affected the health outcomes of all or some their patients.
Financial instability (34% of patients) and transportation problems (24% of patients) were the top two social drivers of health experienced by physicians’ patients.
A solid majority of physicians (80%) reported that addressing social drivers of health is essential to improve health outcomes and decrease healthcare costs.
From the Rx coverage front, the FEHBlog noticed today that GoodRx has added a telehealth option to its website.
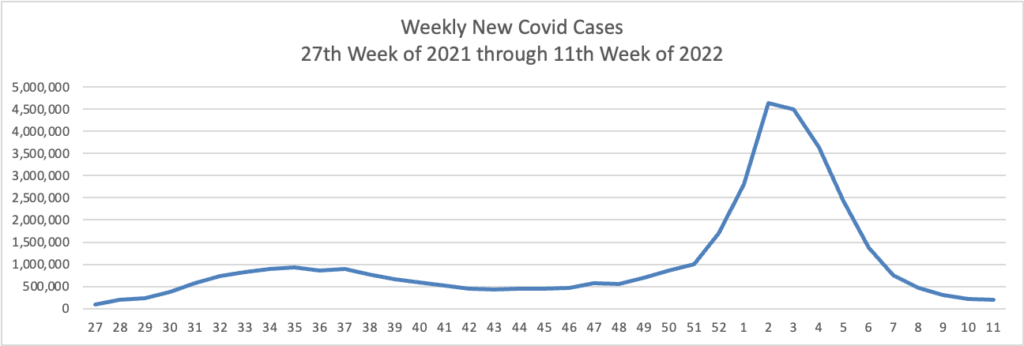
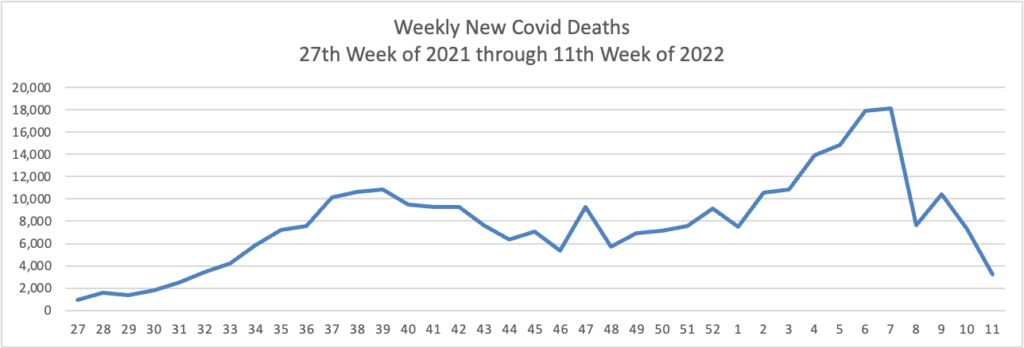
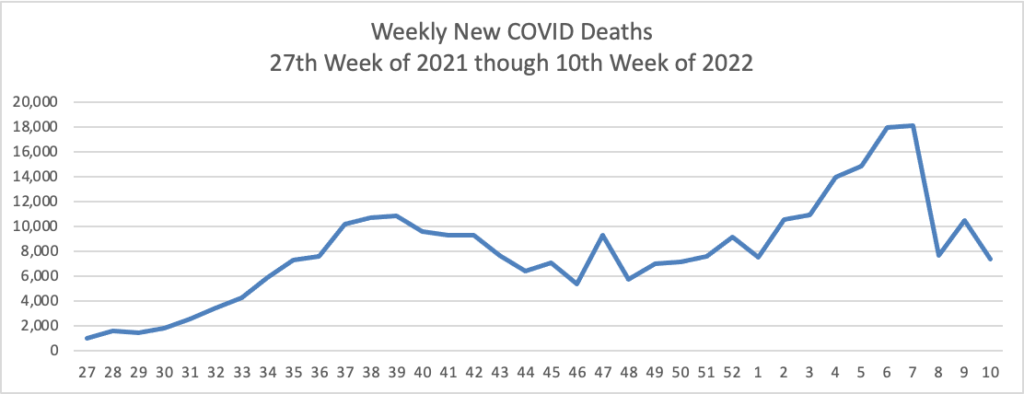
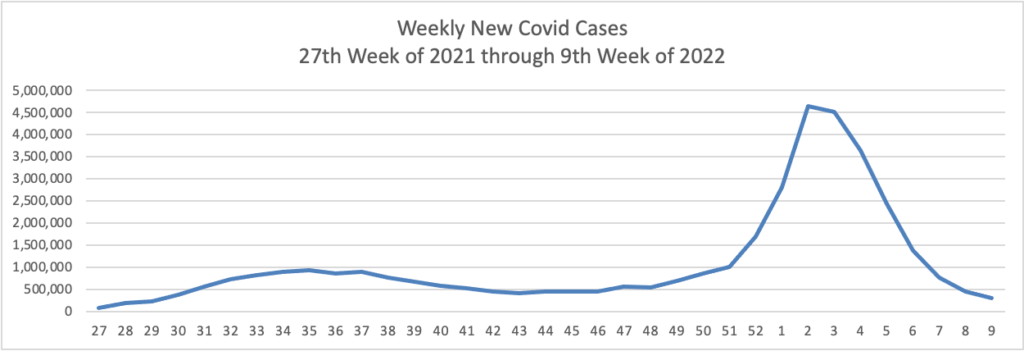
Based on the Centers for Disease Control’s Covid Data Tracker and using Thursday as the first day of the week, here is the FEHBlog’s latest weekly charts of new Covid cases and deaths (a lagging indicator):
The CDC observes in its weekly review of its Covid statistics
COVID-19 cases, hospitalizations, and deaths all continue to decrease in the United States. According to CDC’s COVID Data Tracker, as of March 16, 2022, 76.7% of the total U.S. population has received at least one dose of a COVID-19 vaccine, and 65.3% has completed their primary series. However, only about half of the booster-eligible population has received a booster dose and is considered up to date on their COVID-19 vaccines.
Two new studies show the effectiveness of COVID-19 vaccines and boosters across periods of three variants of concern (Alpha, Delta, and Omicron). CDC released a study today showing that, among adults hospitalized with COVID-19 during the Delta and Omicron waves, those who received two or three doses of the Pfizer-BioNTech or Moderna vaccine had 90–95% less risk of dying or needing a ventilator compared with adults who were not vaccinated. Protection was highest in adults who received a third COVID-19 vaccine dose. A study published in the British Medical Journalexternal icon found that vaccines gave a high level of protection against hospitalization for all variants, but not as much for Omicron among adults who received only a primary series. However, boosters increased protection against Omicron. The study also showed that hospital patients who were vaccinated had much lower disease severity than patients who were not vaccinated.
These studies emphasize the importance of staying up to date with vaccinations—they are our best protection against severe COVID-19 illness. Vaccination is also the safest way to reduce the chance that new variants will emerge. Find a vaccine provider and get your booster dose as soon as you can.
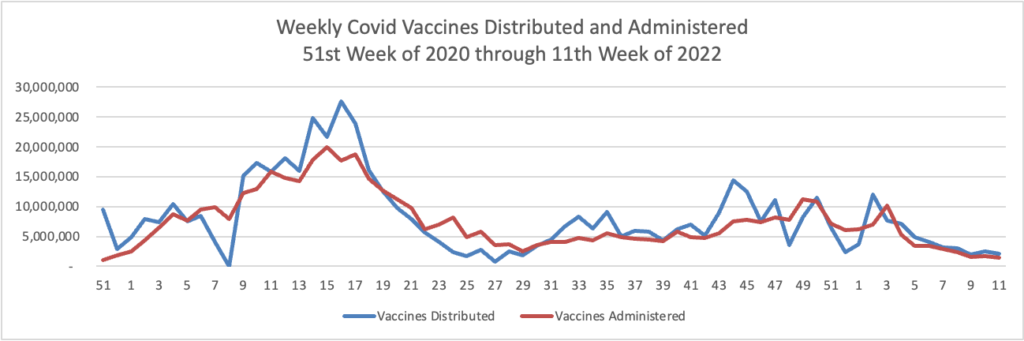
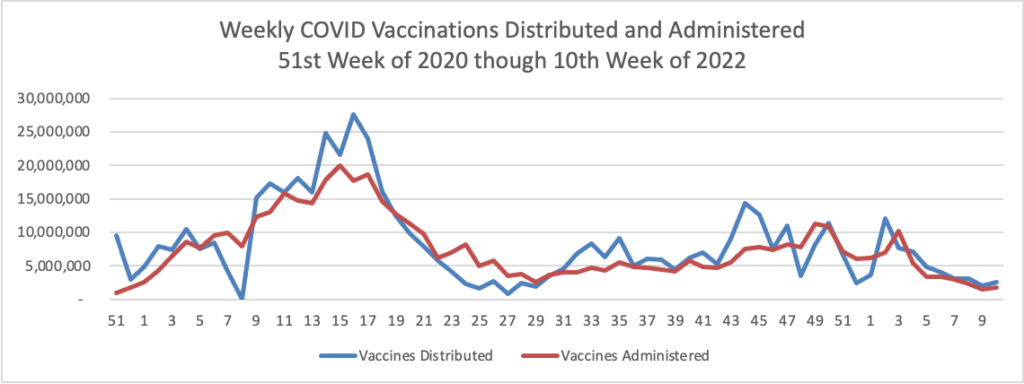
In that regard, here is the FEHBlog weekly chart of Covid vaccinations distributed and administered from the beginning of the vaccination era in late 2020:
Here’s a link to the Food and Drug Administration’s March 18 round of its Covid related activities.
While the bulk of Covid care spending goes to hospitals, Becker’s Hospital Review reports that a “sizable minority” have a significant amount out-of-pocket spending for this care, according to a study published in the American Journal of Managed Care March 16.”
It’s worth adding that the Wall Street Journal reports that
The biggest credit-reporting firms will strip tens of billions of dollars in medical debt from consumers’ credit reports, erasing a black mark that makes it harder for millions of Americans to borrow.
Equifax Inc., ExperianPLC and TransUnion are making broad changes to how they report medical debt beginning this summer. The changes, which have been in the works for several months, will remove nearly 70% of medical debt in collections accounts from credit reports.
Beginning in July, the companies will remove medical debt that was paid after it was sent to collections. These debts can stick around on a consumer’s credit report for up to seven years, even if they are paid off. New unpaid medical debts won’t get added to credit reports for a full year after being sent to collections.
The firms are also planning to remove unpaid medical debts of less than $500 in the first half of next year. That threshold could rise, according to people familiar with the matter.
From the compliance front —
The Internal Revenue Services issued a notice on how to calculate the No Surprises Act’s Qualified Payment Amount when the health plan does not have enough data to calculate a January 2019 median.
The Department of Labor is offering a webinar on March 30 at 11 am that “will help employers, service providers, and benefit professionals understand how the provisions of [the federal mental health partity act] apply to employer-sponsored group health plans and provide information on how to avoid common problems. The webinar runs about 45 minutes to an hour and is limited to 200 participants.
From this week’s healthcare conferences front
Fierce Healthcare discusses the electronic medical records interoperability theme of the HIMSS conference.
Fierce Healthcare also offers a wrap report on “the most interesting innovations at SXSW 2022: From holograms to the future of psychedelics.”
From the telehealth front
Becker’s Payer Issues reports that most consumer driven plans have taken advantage of the IRS offered flexibility to cover telehealth before the “high” annnual deductible.
Forbes informs us “Telehealth Accounts For One In Three Mental Health Visits Two Years Into Pandemic.” Whoopee.
From the good works department, the American Medical Association tells us about a North Carolina physician who is talking the diabetes problem.
Dr. [Brian] Klausner is the medical director of WakeMed’s Community Population Health program in Raleigh. He also is a physician champion for DiabetesFreeNC. That is the statewide initiative where AMA partnered with the North Carolina Medical Society and others to support collaborative efforts to end type 2 diabetes in the Tar Heel State.
Rather than think of the pandemic as having “derailed” diabetes prevention or other population health efforts, Dr. Klausner said that “COVID-19 expedited new perspective in how we can do a better job addressing historic roadblocks to community health initiatives, including those related to diabetes and prevention.”
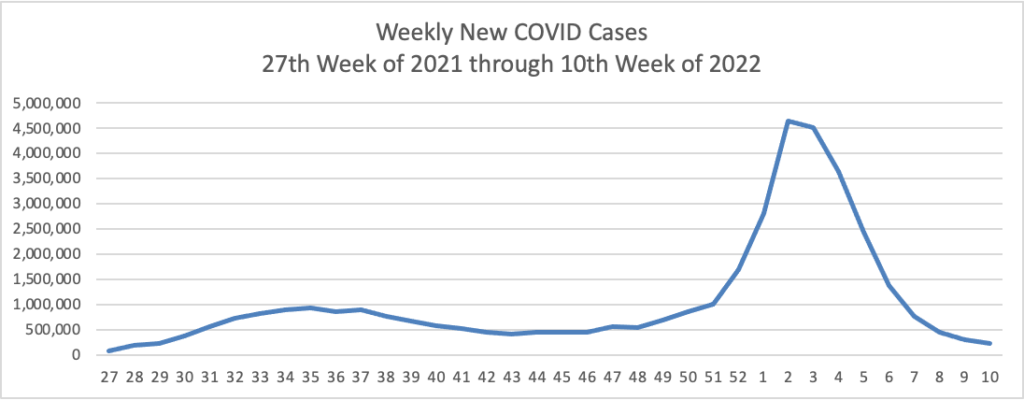
Based on the Centers for Disease Control’s Covid Data Tracker and using Thursday as the first day of the week, here is the FEHBlog’s updated weekly chart of new Covid cases:
Not quite as low as we were in early July but very much moving in the right direction. So is the FEHBlog’s updated weekly chart of new Covid deaths, which is considered a lagging indicator.
The epidemiologists have a keen eye out for new worrisome variants. For example, for other troubling variants, Becker’s Hospital News tells us about a relatively new combination of Delta and Omicron known as Deltacron.
The recombinant variant appears unlikely to spread as easily as delta or omicron, William Lee, PhD, vice president of science at Helix, told USA Today. “We have not seen any change in the epidemiology with this recombinant,” WHO COVID-19 technical lead Maria Van Kerkhove, PhD, said of deltacron during a March 9 media briefing. “We haven’t seen any change in severity. But there are many studies that are underway.”
Here’s the FEHBlog’s weekly chart of Covid vaccinations distributed and administered from the start of the Covid vaccination era in late 2020 until the week ended this past Wednesday.
It is noteworthy that this week, the percentage of Americans aged 18 and older who are fully vaccinated (two doses of mRNA vaccine) cracked 75%. The same cadre is closing in on being 50% boostered. The most at risk, over age 65 cadre is 89% fully vaccinated and 66.7% boostered.
In a study of 1,364 children aged 5-15, two doses of the Pfizer COVID-19 vaccine reduced the risk of omicron infection by 31% in those under 12 and 59% in older children, the Centers for Disease Control and Prevention reported today. CDC said the study reinforces the importance of vaccination to keep children and teens protected from severe disease, noting that another recent study found the vaccine 92%-94% effective against COVID-19 hospitalization in adolescents during the delta surge and 74% effective against hospitalization in younger children during omicron.
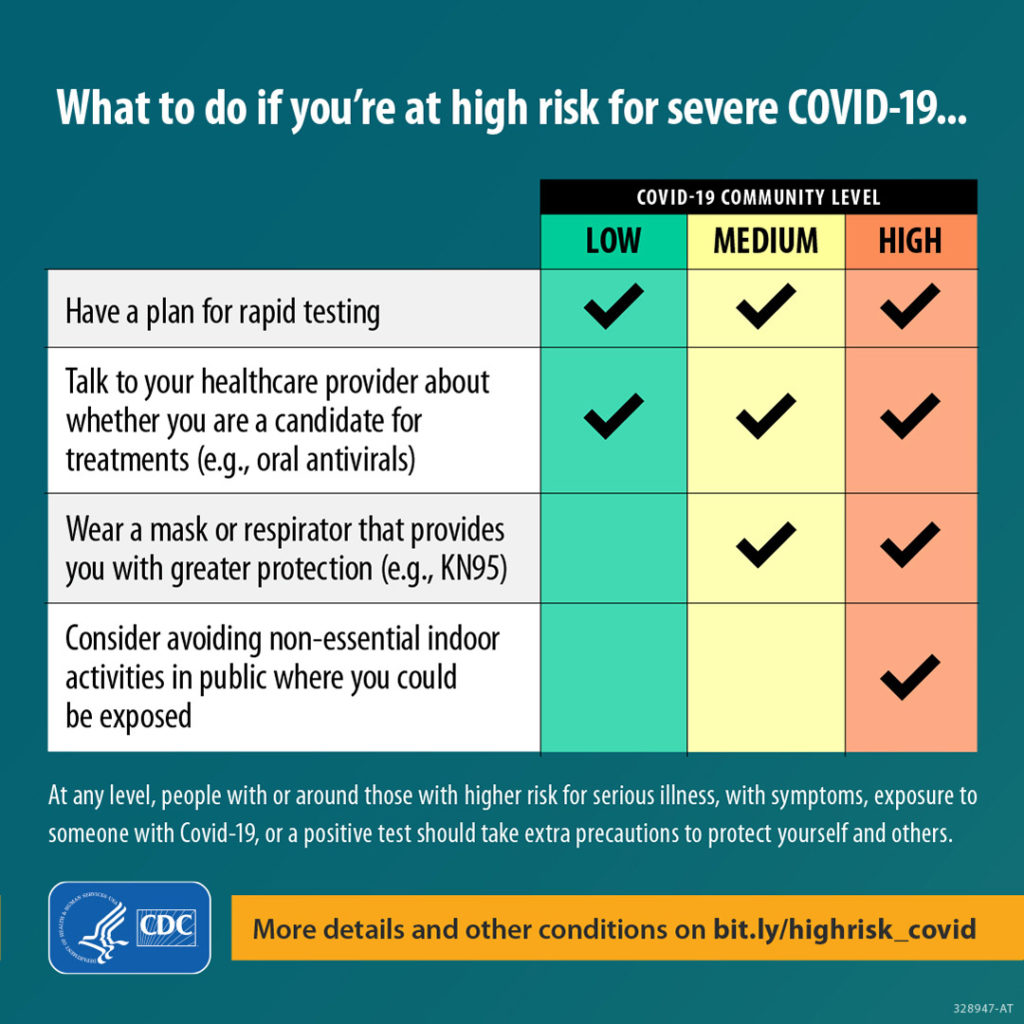
Here’s a link to the CDC’s weekly review of its Covid statistics. This week’s issue focuses on protecting folks at high risk for Covid, such as the immunocompromised.
Who is most likely to become very sick or die from COVID-19? Your chances increase with age and underlying medical conditions like cancer, diabetes, heart conditions, dementia, and obesity, particularly if you’re not up to date on vaccinations. People with weakened immune systems,* some disabilities, some mental health conditions, and some chronic diseases are also at higher risk. A lot of people might not know they’re at risk for severe illness—review the list to find out if you could be.
Here’s a link to the CDC’s weekly Fluview report, which states that flu activity is increasing in “most of the country.” In this regard, the American Medical Association inform us
Healio (3/10, Downey, Gallagher) reports “interim estimates published Thursday in” the CDC’s Morbidity and Mortality Weekly Report “indicate that this season’s influenza vaccine has not been effective.” Based on the data “from more than 3,600 children and adults,” researchers “estimated that the vaccine has been 16% effective against mild or moderate influenza caused by the predominant circulating virus, influenza A(H3N2), with a 95% confidence interval…that suggests vaccination ‘did not significantly reduce the risk of outpatient medically attended illness’ caused by H3N2.”
From Capitol Hill and closing the loop on Thursday’s post, the Senate did pass the fiscal year 2022 omnibus appropriations act Thursday night. Roll Call reports
On a 68-31 vote, the Senate passed the 2,700-page, $1.5 trillion omnibus containing all 12 fiscal 2022 spending bills, $13.6 billion in supplemental appropriations to address the crisis in Ukraine and a lengthy list of unrelated measures fortunate enough to ride on the must-pass vehicle.
From the No Surprises Act front, the FEHBlog had been concerned that the federal regulators were giving up on using the Qualified Payment Amount as a rebuttable presumption in NSA arbitrations which would help tremendously to control out of network benefit and plan legal costs. The FEHBlog therefore was encouraged to find that the federal government has filed a brief with the federal district court for the District of Columbia defending that position in a case raising the same issue. An oral argument on this issue will be heard by District Judge Richard Leon on March 21, 2022, at 3 pm. The FEHBlog will keep an eye on this and the other federal cases raising this issue.
From the electronic health record front, MedCity News interviews the CEO of Epic Systems at the Vive conference. The interview covers interoperability, artificial intelligence and other timely topics.
From the opioid epidemic front, STAT News reports
It was in the mid-2010s, the researchers heard, when “tranq dope” — opioids that contained the veterinary tranquilizer xylazine — took off in Philadelphia. But now, in some places across the U.S., it was appearing in 1 in 5 overdose deaths. A recent study also found the powerful synthetic opioid fentanyl in nearly every xylazine-involved death as well, indicating it wasn’t just the tranquilizer causing these overdoses. Experts are still trying to understand the risks of xylazine, but they’re worried because the drug is not an opioid but acts as a sedative, which can increase the risk of a fatal overdose. It might also make it harder to reverse those overdoses with naloxone, which is designed to work on opioids. STAT’s Andrew Joseph has more on how adulterated — and in turn, increasingly dangerous — the U.S. drug supply has become.
The Senate has locked in a deal to quickly pass a massive government funding bill that includes $13.6 billion in Ukraine aid.
The agreement, announced by Senate Majority Leader Charles Schumer (D-N.Y.), puts the funding bill on a glide path to pass on Thursday night, capping off hours of would-they-won’t-they drama.
Mazaal tov to Congress.
Also on Capitol Hill today, the Senate Homeland Security and Governmental Affairs Committee held a confirmation hearing for Krista Boyd, the President’s nominee to serve as OPM Inspector General. Fedweek notes that “Ms. Boyd is a senior staff member of the House Oversight and Reform Committee with long experience on Capitol Hill in federal workplace matters.”
From the Omicron front, Becker’s Hospital Review informs us “The rate of new COVID-19 cases involving the omicron subvariant BA.2 appears to be slowing in the U.S., according to variant proportion estimates from the CDC.”
Also, the Justice Department announced “Effective immediately, Associate Deputy Attorney General Kevin Chambers will serve as the Director for COVID-19 Fraud Enforcement.”
From the litigation front, Reuters reports “The judge overseeing Purdue Pharma’s bankruptcy on Wednesday approved a $6 billion opioid settlement funded by its Sackler family owners, overruling objections from the Department of Justice and 20 states that opposed the deal.”
Anthem plans to change its name to Elevance Health, if the move is approved by shareholders, the company said Thursday.
The new name is meant to reflect the company’s offerings beyond traditional health insurance. “Elevance Health’s companies will serve people across the entire care journey, connecting them to the care, support, and resources they need to lead healthy lives,” Anthem CEO Gail Boudreaux said in a statement.
Elevance was chosen as a combination of the words “elevate” and “advance.” There will not be any changes to leadership or organizational structure accompanying the new name.
If approved, the Elevance name will start being used at the end of the second quarter of this year. Anthem Blue Cross and Blue Shield plans will still use the Anthem name.
From the telehealth front, Healthcare Dive reports
[Virtual care vendor] Amwell and LG Electronics are teaming up to jointly develop new digital health devices and tools, starting with hospital care in the U.S., the companies announced Wednesday.
South Korea-based LG, which manufactures a wide range of devices from refrigerators to computer monitors, already provides smart TVs for inpatient rooms.
Now, through the partnership, LG will also create devices that can host services from Amwell’s virtual care platform, Converge.
PYMTS.com reports this electronic health records news from the Vive conference being held in Miami
Electronic health records containing some of the most guarded personal data about people are making headlines again as a consortium of players join forces to create a universal single sign-in, allowing patients secure access to unified health data via digital identity.
Coming out of the ViVE health technology conference happening this week in Miami Beach, the effort is led by consumer-directed healthcare advocacy group the CARIN Alliance, working together with the Department of Health and Human Services (HHS) and other stakeholders.
On Tuesday (Mar. 8), Politico reported that HHS “is working with several health systems, insurers and health tech groups to roll out a single way for patients to log in and access their medical records across multiple systems. The launch later this month will set up a test environment for integrating the technology, said Ryan Howells, principal at Leavitt Partners and program manager at the CARIN Alliance, which is spearheading the efforts.”
CARIN is working with the Office of the National Coordinator for Health Information Technology and the Centers for Medicare and Medicaid Services (CMS), which will act as “government observers.”
From the FEHB front, benefits consultant Tammy Flanagan writes in Govexec about the Postal Service Health Benefits Program which will launch in 2025 as part of the Postal Reform Act of 2022. She observes
The version of the postal bill that eventually passed balances the risk pools, and the Office of Personnel Management now estimates premiums should go down for postal and non-postal employees and retirees alike.
The new law keeps all postal workers in FEHB, in their own group. All workers will be able to keep their current plans and avail themselves of the annual open season to choose other options within FEHB.
Future postal retirees will be required to enroll in Medicare A and B at 65. Retiree health coverage will then become a combination of Medicare and FEHB.
The question now is whether that requirement will eventually be extended to all federal employees, and what effect that would have on the premiums retirees pay. If that happens, at least federal employees will face one less tough decision at the time of retirement.
The FEHBlog expects that PSHBP premiums will be materially lower than FEHB premiums because PSHBP will accept Medicare funding for prescription drug benefits in the form of Part D EGWPs. Federal law has permitted the FEHB to offer premium-reducing Part D EGWPs for nearly twenty years. Nevertheless, OPM and a string of Administrations from George W. Bush to Joe Biden have refused to implement that law. Implementing that law in 2005 when it first took effect likely would have avoided the balkanization of the FEHB that we will soon experience with the PSHBP.
The FEHBlog does not expect the FEHB to adopt the mandatory Part B approach being taken by the PSHBP. Fewer retiring federal employees are picking up Part B because of the income-adjusted Part B premiums. As basic and income-adjusted Part B premiums continue to climb and climb, the FEHBlog expects that the PSHBP will liberalize, and then do away with, mandatory Part B. Meanwhile, the PSHBP’s undoubtedly favorable experience with Medicare funding of prescription drugs will lead OPM to allow FEHB the same opportunity.
With both branches of the Program using Part D EGWPs and integrated Medicare Advantage plans, everyone will enjoy reasonable premiums for high-quality healthcare. That in turn could lead to a reunion of the two branches. Hopefully, the PSHBP will be a relatively brief experiment that leaves the FEHB Program stronger.
The saving grace of the FEHB Program is that everyone in a plan option pays the same premium and the premiums are pooled to cover all plan option enrollees. That’s the bedrock principle of group health insurance that the FEHB Program has shown to work.
From Capitol Hill, the Senate late this afternoon agreed by a 74-17 vote to end debate on the Postal Reform Act of 2022 (H.R. 3076). “The Senate stands in recess until 10:30 am on Tuesday, March 8, 2022. Following Leader remarks, the Senate will resume consideration of Calendar #273, H.R. 3076, Postal Service Reform Act, post-cloture.” The time for the final Senate vote on H.R. 3076 is yet to be determined. Senate passage, which requires a simple majority vote, is assured.
Federal News Network calls attention to the fact that a month ago today the White House issued a statement of administration policy on H.R. 3076 which reads in pertinent part
H.R. 3076 would also establish a new, separate Postal Service Health Benefits Program (PSHBP) within the existing Federal Employees Health Benefits Program (FEHBP), that integratesPostal employees and annuitants into Medicare. Making these changes would improve the Postal Service’s long-run financial outlook, without sacrificing quality, affordable healthcoverage for Postal employees and retirees. The Administration is mindful that these reforms wouldimpose administrative burdens on the Office of Personnel Management and FEHBP, and further,that there could be potential challenges with operationalizing Medicare integration and withensuring ongoing funding to support administration of the new PSHPB. The Administration looks forward to working with Congress to ensure that the goals of H.R. 3076 are met in anefficient, equitable, and cost-effective manner, while safeguarding the continued stability of the FEHBP
Top appropriators and congressional leaders are aiming to wrap up omnibus negotiations within 24 hours so they can file the massive spending package in the House on Tuesday, vote on it in that chamber Wednesday and get it through the Senate before Friday at midnight when stopgap funding expires.
While so-called open items remained, there was confidence on both sides of the aisle that talks were going well enough on the massive, long-overdue package that a fourth continuing resolution for the fiscal year that began Oct. 1 wouldn’t be necessary.
A new report released Monday charts a path for the transition out of the Covid-19 pandemic, one that outlines both how the country can deal with the challenge of endemic Covid disease and how to prepare for future biosecurity threats.
The report plots a course to what its authors call the “next normal” — living with the SARS-CoV-2 virus as a continuing threat that needs to be managed. Doing so will require improvements on a number of fronts, from better surveillance for Covid and other pathogens to keeping tabs on how taxed hospitals are; and from efforts to address the air quality in buildings to continued investment in antiviral drugs and better vaccines. The authors also call for offering people sick with respiratory symptoms easy access to testing and, if they are positive for Covid or influenza, a quick prescription for the relevant antiviral drug.
The 136-page report was written by nearly two dozen experts, a number of whom have advised the Biden administration on its Covid-19 policies. Thirty other experts contributed to the report, entitled “Getting to and Sustaining the Next Normal: A Roadmap to Living with Covid.”
Helpful. Speaking of which, the Centers for Disease Control offers advice on how to prepare children and teens for Covid vaccination.
From the healthcare cost front, Healthcare Dive reports
Higher-priced emergency care was associated with lower mortality in hospital markets with less hospital concentration, but survival rates were similar for low- and high-priced hospitals in more concentrated markets, according to a working paper released last week from the nonprofit National Bureau of Economic Research.
The researchers determined that additional spending on quality improvements at expensive hospitals in unconcentrated markets is potentially cost-effective.
However, they found no evidence of better outcomes among patients admitted for emergency care to pricier hospitals in markets with less competition, despite substantially higher costs. “In these concentrated markets, high prices likely reflect patients’ lack of alternative options, not hospital quality,” the study said.
From the healthcare business front, Fierce Healthcare tells us
GoodRx is scooping up vitaCare Prescription Services from TherapeuticsMD to beef up its growing pharma manufacturer solutions business.
VitaCare is a technology and services platform designed to make the complex process of filling prescriptions simple, cost-effective and stress-free for patients.
In recent months, the COVID-19 pandemic has highlighted the value of pharmaceutical companies being able to connect directly with patients, according to TherapeuticsMD in its latest earnings release. This in combination with the rise of interest and investment in other hub service and pharmacy services companies has driven outside interest in vitaCare both from pharmaceutical companies seeking to utilize vitaCare for their products and from potential partners or sponsors seeking to acquire a controlling interest in vitaCare.
GoodRx has agreed to acquire vitaCare for $150 million in cash, with an additional $7 million consideration contingent upon vitaCare’s financial performance through 2023, according to the companies.
The transaction is expected to close in mid-2022.
From the telehealth from, HR Tech shares large employer tips on how to promote employee use of telehealth or as its now called virtual care.
March is Women’s History Month, and the Veterans Administration gives us a chance to virtually meet several VA oncologists, some of the women who are making cancer history.
Based on the Centers for Disease Control’s Covid Data Tracker and using Thursday as the first day of the week, here is the FEHBlog’s latest weekly chart of new Covid cases
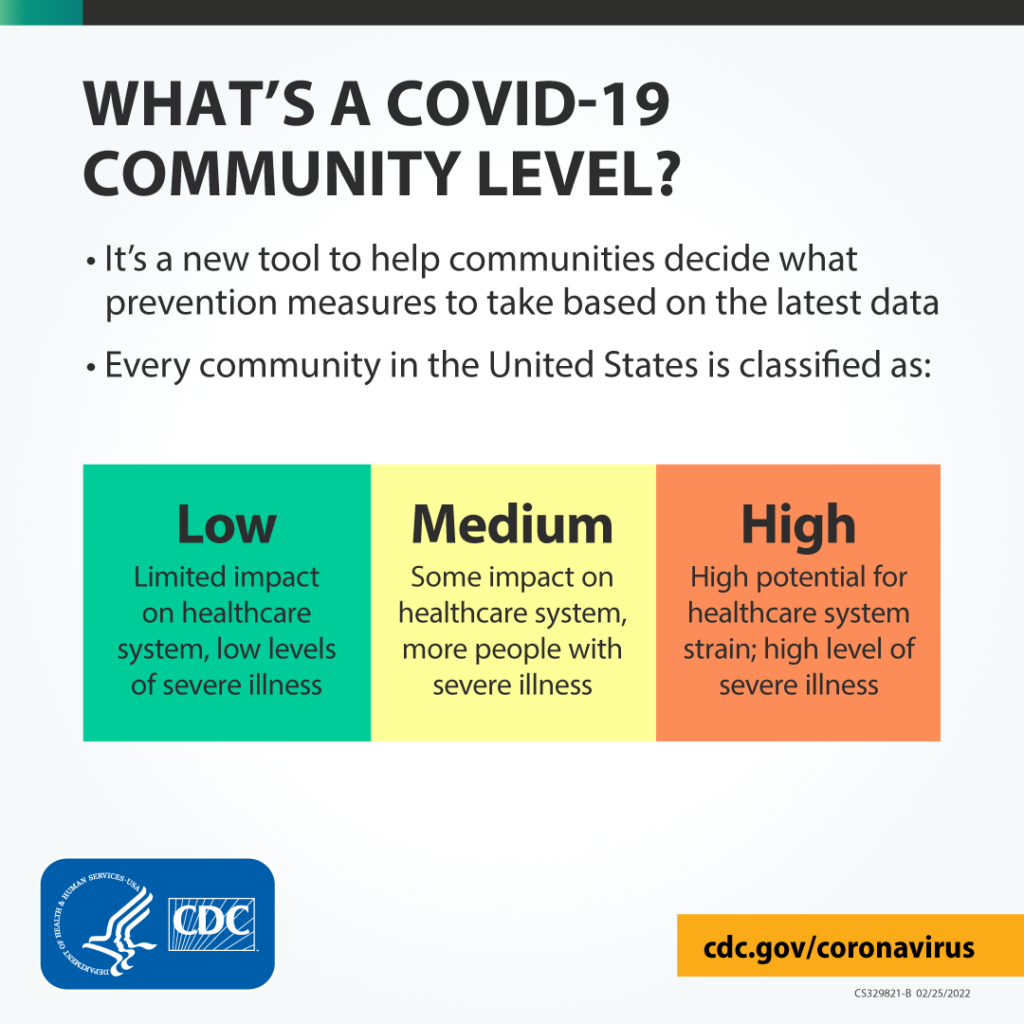
The Centers for Disease Control and Prevention yesterday said more than 90% of the U.S. population now lives in a county with a low or medium COVID-19 Community Level, a new CDC measure for communities considering whether to require face coverings in public indoor settings. The agency plans to update the county data every Thursday going forward.
Cases of the highly transmissible omicron subvariant appear to be doubling every week in the U.S., but there isn’t clear evidence BA.2 will cause another major surge, epidemiologist Michael Osterholm, PhD, told Becker’s March 2. * * *
Cases will likely continue to drop over time, Dr. Osterholm said, adding he is hopeful cases will reach or fall below levels not seen since last June, when the nation’s new case average fell below 12,000.
It’s worth noting that the FEHBlog weekly chart of new cases found above begins with the low point Dr. Osterholm references, new cases under 12,000 and new deaths under 1,000.
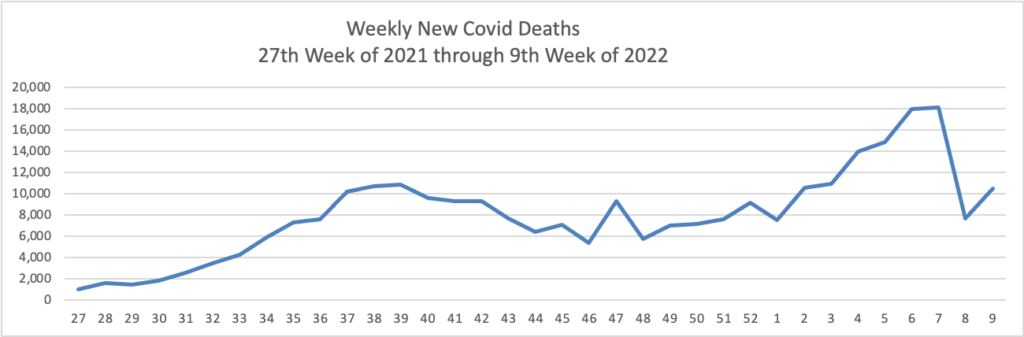
Here’s the FEHBlog’s weekly chart of new COVID deaths
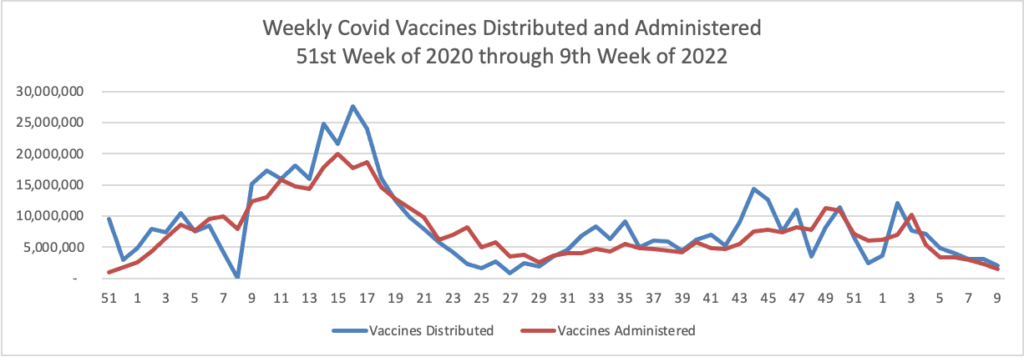
Here’s the FEHBlog’s weekly chart of Covid vaccinations distributed and administered from the 51st week of 2020 through the 9th week of 2022
From the Covid vaccine front, Bloomberg informs us
Parents still hesitating to get their kids vaccinated may be reassured by reporting that shows Covid inoculations protected children and teenagers from severe disease, even after the rise of the immune-evasive omicron variant.
Omicron came to the U.S. late last year armed with some 30 mutations in its spike protein that make it less recognizable to immune antibodies. Afterward, vaccine protection against infection and urgent care visits declined for 5- to 17-year-olds who’d received primary inoculations, according to U.S. Centers for Disease Control and Prevention data released Tuesday. However, vaccinated children and teens were still less likely to get infected than their unvaccinated peers, the agency said in its Morbidity and Mortality Weekly Report.
The CDC released recommendations last week saying that schools in areas of low and moderate risk can drop indoor mask mandates, the first update to its guidance on the topic since July — and the new findings may add confidence in moves to relax social measures as infections fall across the U.S. But many parents have been slow to get shots for their kids since the vaccine was recommended in November, and vaccinations among kids ages 5 to 11 have fallen to their lowest levels since the shots were first cleared.
While kids generally don’t get as sick as adults from the coronavirus, clearing a vaccine for elementary school-age children marked a major milestone in the pandemic. It provided peace of mind for many concerned parents, allowing kids to resume activities that had been on hold since the virus first began spreading in the U.S.
Pfizer and BioNTech’s is the only shot that has been authorized for use in U.S. children and teens. The CDC looked at vaccine protection against infection, urgent care visits, hospitalization, and death among vaccinated children ages 5 through 11 and adolescents ages 12 through 17 before and during the omicron surge.
That’s solid information for health plans to share with their members.
Here’s a link to the CDC’s Weekly Review of its Covid statistics. Beckers Hospital Review saves you time by breaking down those stats at this link.
The CDC’s weekly FluView tells us “Sporadic influenza activity continues across the country. In some areas, influenza activity is increasing.”
Negotiations over an omnibus spending package remained far from complete Thursday as the late arrival of a White House supplemental funding request threw a wrench in the talks.
The White House on Thursday formally asked lawmakers to attach to the fiscal 2022 spending package $32.5 billion in emergency funds for government response efforts to the ongoing COVID-19 pandemic and Russian war with Ukraine.
The long-awaited details from the administration on its justification for the extra spending, on top of the roughly $1.5 trillion expected to be appropriated for the current fiscal year, come barely a week before stopgap funding expires March 11.
To pass the omnibus before that deadline, Senate Appropriations ranking member Richard C. Shelby, R-Ala., said lawmakers need to get a final deal by Tuesday — and even that may be too late to avoid the need for another short-term continuing resolution.
“We made good progress this week. But we make progress and we’re stalled,” he said. “And we can’t afford to stall this weekend. If we do, we’re headed for a CR.”
From the SOTU front, AHIP released AHIP President Matt Eyles’s comments on the President’s address.
From the health equity front, Mercer Consulting released a report finding a surprising gender gap in employer-sponsored health benefits continues to exist.
Based on the Centers for Disease Control’s (CDC) Covid Data Tracker website and using Thursday as the first day of the week, here are the FEHBlog’s charts of weekly new Covid cases and deaths from the 27th week of 2021 through the 8th week of 2022, both of which are plummeting
Here’s the FEHBlog chart of weekly Covid vaccinations distributed and administered from the 51st week of 2020 through the 8th week of 2022iew
Here are links to the CDC’s weekly review of its Covid statistics and its weekly Fluview. The Covid news is significant
CDC is updating the way it monitors COVID-19’s impact on our communities. Widespread availability of vaccines and testing, advances in treatments, and increasing levels of immunity in the population through vaccination or previous infection have moved the COVID-19 pandemic to a new phase. While we can’t prevent all cases of COVID-19, we can continue to limit the spread and protect those who are most at risk of severe illness.
Given this new phase of the pandemic, CDC is launching a new tool to monitor COVID-19 Community Levels. Each county’s COVID-19 Community Level is ranked as low, medium, or high (find your county’s level). The COVID-19 Community Level map where you can find your county’s level will be updated regularly with new data.
As of now, most counties in the country fall into either low-risk or medium-risk categories, said Greta Massetti, PhD, of the COVID-19 Response Incident Management Team.
Those counties, “representing 70 percent of Americans, are in low to medium community levels,” she said. “We continue to see indicators improve in many counties.”
A total of 23% of U.S. counties fall into the low-risk group, and 39% are medium-risk, Massetti said.
But, Walensky said, these guidelines could change at any time if numbers begin moving in the wrong direction.
Also, from the policy front
Medscape tells us and as evidenced by the new CDC approach
The White House has begun a sweeping overhaul of its COVID-19 strategy as the U.S. moves out of pandemic crisis mode and into a more manageable phase, according to ABC News.
The new strategy is expected to acknowledge that the coronavirus is becoming a less urgent threat to Americans overall due to access to vaccines, testing, and therapeutics.
Insurance News Net informs us about AHIP’s 2022 priorities as identified by its President Matt Eyles:
Affordable coverage, improved access. Addressing the underlying cost drivers of care. Ending pharma monopolies. Addressing hospital and physician group consolidation. Pushing back on restrictions on medical management.
Improving health equity. Ensuring everyone has an equal opportunity to thrive and achieve their best possible health. Expanding initiatives to provide health care opportunities to underserved areas and populations. Providing COVID-19 vaccine outreach to at-risk older Americans. Providing outreach in a culturally competent manner to various ethnic groups.
Post-pandemic health care. AHIP will develop a post-pandemic road map to improve health care. AHIP is working to maintain coverage for those who were eligible for coverage under Medicaid or the Affordable Care Act during the public health emergency so that they will continue to have coverage when the emergency ends.
Improving competition and choice. Maintain a competitive private health insurance market.
Worthy priorities, indeed.
Fierce Healthcare tells us about the American Medical Association’s President’s speech on the AMA priorities for improving U.S. healthcare and readiness for future pandemics.
From the avoiding low-value care front, Medscape reports
Low-value healthcare services that provide little or no benefit to patients are “common, potentially harmful, and costly,” and there is a critical need to reduce this kind of care, the American Heart Association (AHA) says in a newly released scientific statement.
Each year, nearly half of patients in the United States will receive at least one low-value test or procedure, with the attendant risk of avoidable complications from cascades of care and excess costs to individuals and society, the authors note.
Reducing low-value care is particularly important in cardiology, given the high prevalence and costs of cardiovascular disease in the United States, they note.
The statement was published online February 22 in Circulation: Cardiovascular Quality and Outcomes.
From the mental healthcare front, Health Affairs Forefront discusses how
This July, the US model for responding to individuals experiencing a mental health crisis is scheduled for a much-needed change. The 988 number is a three-digit, national mental health crisis hotline that was mandated by the federal government in October 2020 with an official nationwide start date on July 16, 2022. * * *
The 988 hotline holds incredible promise toward decriminalizing the response to mental health emergencies. Currently, if an individual is experiencing a mental health crisis, they, their caregivers, and bystanders have few options beyond calling 911. As a result, roughly one in 10 individuals with mental health disorders have interacted with law enforcement prior to receiving psychiatric care, and 10 percent of police calls are for mental health emergencies. * * *
Ideally, the new 988 number would activate an entirely different cascade of events. An individual in crisis, their family member, or even a bystander will be able to immediately reach a trained crisis counselor who can provide phone-based triage, support, and local resources. If needed, the counselor can activate a mobile mental health crisis team that will arrive on site to de-escalate; provide brief therapeutic interventions; either refer for close outpatient follow up or transport the individual for further psychiatric evaluation; and even offer food, drink, and hygiene supplies.
That’s an interesting perspective. Health plans should plan to publicize the 988 number this summer.
From the chronic disease front, Health Payer Intelligence uses a recent CMS report on healthcare spending to identify the ten most expenses chronic diseases in our country.
From the Rx coverage front, Healthcare Dive reports
The Federal Trade Commission is calling on the public to submit feedback on how pharmacy benefit managers’ business practices are affecting patients, pharmacies and employers.
The agency is seeking to gather a wide range of information and comments on pharmacy benefit managers, including how they affect drug prices, access, contract terms, rebates, fees, steering methods, conflicts of interest and consolidation, according to the request for information released Thursday.
Members of the public can comment through April 25. The information the FTC collects will enable the agency to “study a wide array of PBM business practices and issues and will help inform the agency’s policy and enforcement work,” the regulator said in a statement.
Finally in litigation news, the Wall Street Journal informs us
Pharmaceutical company Johnson & Johnson and three of the nation’s biggest drug distributors have agreed to move forward with a landmark settlement with a majority of states, bringing thousands of lawsuits over the opioid epidemic closer to the finish line.
Drug distributors AmerisourceBergen Corp. , Cardinal Health Inc. and McKesson Corp. would pay a total of $19.5 billion to 46 states over 18 years, according to the companies. Johnson & Johnson said it would pay $5 billion to 45 states.
The global settlement was first announced last summer. It was given final approval by the companies after a threshold number of state and local governments agreed to participate and currently amounts to roughly $25 billion.
The settlement is the largest to date from more than 3,000 lawsuits brought by states, local governments, Native American tribes, hospital groups and others alleging that companies from pharmaceutical manufacturers to distributors and pharmacies flooded areas with pills and created the opioid epidemic, ultimately forcing communities to spend millions of dollars responding to the crisis.
Let’s hope that the settlement funds are used to end our other national epidemic, substance use disorder.
Let’s start today with news from the litigation front —
The Wall Street Journal reports that in advance of the February 27 deadline,
The Justice Department filed an antitrust lawsuit Thursday challenging UnitedHealth Group Inc.’s$13 billion acquisition of health-technology firm Change Healthcare Inc., arguing the tie-up would unlawfully reduce competition in markets for commercial insurance and the processing of claims.
The deal, announced in January 2021, sought to bring a major provider of healthcare clinical and financial services, including the handling of claims, under UnitedHealth’s Optum health-services arm.
The Justice Department filed its lawsuit in federal court in Washington, saying Change provided key industry technologies that are relied upon by UnitedHealth’s health-insurance rivals, making it a hub for competitively sensitive information. If the deal were allowed, UnitedHealth would have access to data that it could potentially use for its own benefit, at the expense of other insurers, the department alleged. The department also argued the deal would reduce head-to-head competition in the businesses of insurance claims transmission and review, because UnitedHealth competes with Change in those areas.
A federal judge in Texas struck down a narrow part of the surprise billing rule that outlines how to resolve payment disputes between payers and providers over out-of-network claims. Wednesday’s ruling is a win for providers who were opposed to the dispute resolution process spelled out by CMS in an interim rule, arguing it favored insurers.
The judge’s ruling essentially tosses out a part of the dispute resolution process that instructs arbiters to begin with the presumption that the qualifying payment amount, or median in-network rate, is the appropriate payment amount for providers.
This is not the final word because the decision, which resulted in a final judgment is appealable to the U.S. Court of Appeals for the Fifth Circuit. A case raising the same issue is currently pending oral argument in the U.S. District Court for the District of Columbia.
Katie Keith, a health law expert at Georgetown University, said the ruling is evidence of how hard doctors groups will fight even relatively modest efforts by Congress to cut health care costs.
The surprise billing action was “one of the few things Congress has tried to do on cost containment,” she said.
Amen to that.
From the Omicron front, Medpage Today provides background on a Centers for Disease Control decision permitting
Extended dosing intervals for Pfizer or Moderna vaccines * * * for certain individuals ages 12 to 64 years, not only to lower the risk of vaccine-associated myocarditis, but to potentially improve vaccine effectiveness, CDC staff said on Thursday.
According to the agency’s new interim guidance, young people ages 12 to 39 may especially benefit from a second mRNA dose 8 weeks after their first dose.
However, the regular 3-week interval for Pfizer and 4-week interval for Moderna is appropriate for patients who are moderately to severely immunocompromised, adults ages 65 and up, those who need rapid protection (such as “during high levels of community transmission”), and children ages 5 to 11.
From the social determinants of health front, HR Dive tells us
Though employers have invested increasingly in a variety of healthcare and healthcare-adjacent benefits, few of these efforts effectively address social determinants of health that can negatively affect patient outcomes, according to a report published this month by the Northeast Business Group on Health.
Social determinants of health include factors such as education access and quality; healthcare access and quality; economic stability; neighborhood and built environment; and social and community factors. Differences in these areas lead to disparities not only in terms of health outcomes, but also in cost management and general employee health and well-being, NEBGH said.
Employers can start addressing social determinants by collecting survey data on employees’ needs and risk factors, per the report. From there, NEBGH recommended that benefits design focus on equitable benefits access, such as evaluating what percentage of pay their health plans comprise at different pay levels. Other strategies cited include improving health literacy, taking advantage of partnerships and improving organizational culture around health and well-being, among others.
From the Rx coverage front, Fierce Healthcare discusses CVS Health’s annual Drug Trend Report.
CVS Caremark kept overall drug trend for clients to 2.4% over the first three quarters of 2021, marking multiple years of single-digit trend in drug price growth.
The pharmacy benefit management arm of CVS Health also kept its specialty drug trend to single digits through the third quarter, at an industry-low 5.8%, according to the company’s annual Drug Trend Report released Thursday. Caremark found that 35.9% of its clients saw negative specialty trend in 2021.
In addition, 65.3% saw specialty trend under 10%, according to the report.
The article explains how CVS Health accomplished this feat.
From the Medicare front, CMS announced a redesign of its Accountable Care Organization model
that better reflects the agency’s vision of creating a health system that achieves equitable outcomes through high quality, affordable, person-centered care. The ACO Realizing Equity, Access, and Community Health (REACH) Model, a redesign of the Global and Professional Direct Contracting (GPDC) Model, addresses stakeholder feedback, participant experience, and Administration priorities, including CMS’ commitment to advancing health equity.
In addition to transitioning the GPDC Model to the ACO REACH Model, CMS is canceling the Geographic Direct Contracting Model (also known as the “Geo Model”) effective immediately. The Geographic Direct Contracting Model, which was announced in December 2020, was paused in March 2021 in response to stakeholder concerns.
Sanofi and GlaxoSmithKline weathered clinical trial delays for their Covid-19 vaccine, but the partners now have data to support filings seeking regulatory authorizations. Key features of the vaccine may be able to persuade the vaccine hesitant; it may also be well-suited for use as a booster.
This news bears similarities to the reports about the Novavax Covid vaccine already submitted to the Food and Drug Administration for emergency use authorization.
The American Hospital Association informs us
The Food and Drug Administration yesterday listed all over-the-counter COVID-19 diagnostic tests authorized for home use, including links to home use instructions for each test.
Walmart has administered tens of millions of COVID-19 vaccines to date, with 80% delivered in medically underserved communities, the retail giant announced Wednesday.
The company released a report (PDF) looking back at its progress in providing vaccines over the course of 2021. Cheryl Pegus, M.D., executive vice president of health and wellness at Walmart, told Fierce Healthcare the company has focused on connecting with people who may not otherwise have been able to get the shot.
From the health equity front —
The American Hospital Association tells us
The U.S. maternal mortality rate increased to 23.8 deaths per 100,000 live births in 2020 from 20.1 in 2019 as rates for Black and Hispanic women increased, according to data released today by the Centers for Disease Control and Prevention. The maternal mortality rate for Black women was nearly three times the rate for white women. Mortality rates increased with maternal age, with the rate for women aged 40 and over nearly eight times higher than the rate for women under 25.
The AHA’s Better Health for Mothers and Babies initiative offers resources to help hospitals and health systems eliminate maternal mortality and address health disparities for mothers and babies.
What can be more tragic than a baby losing a mother?
Beckers Payer Issues adds from the mental health perspective
Work-sponsored health plans aren’t addressing the growth of loneliness, which leads to employees missing work and decreased productivity, according to data from Cigna’s Loneliness Index shared with Becker’s.
The data, which is slated to be published in the Journal of Organizational Effectiveness: People and Performance, surveyed nearly 6,000 employees between July 16 and Aug. 2, 2019.
Six insights:
1. The widespread presence of loneliness affected 3 in 5 (62 percent) adults before the COVID-19 pandemic. Feelings of loneliness play key roles both in employee health and work performance, according to the study.
2. On average, preventable, stress-related absences caused lonely employees to miss about five more work days than their counterparts who did not identify as lonely.
3. Employees who reported higher levels of loneliness were almost twice as likely to consider quitting their current job than employees who were less lonely.
4. The study estimates that absenteeism and productivity losses tied to preventable loneliness cost employers $154 billion each year.
5. The study said work-based factors like communication, work-life balance and social companionship play key roles in determining employee loneliness. Personal resilience and a feeling of connection outside of the workplace also play a role.
6. Employers looking to combat employee loneliness should consider actions that hit on these factors, including flexible work hours, email “blackout” periods and forming employee resource groups.
From the Black History Month department, Everywell, an at-home testing service, celebrates ten Black pioneers who improved healthcare in our country. Bravo.
From the U.S. healthcare front, Healthcare Finance News reports
Including federal government support, national health spending grew by 3.4% in 2021, according to new data released by Altarum.
This growth in spending, the analysis found, reflected the fact that support from the federal government was strong in 2020, likely in response to the recession caused by the COVID-19 pandemic, and was lower in 2021.
Taking these support dollars out of both 2020 and 2021 estimates, spending growth from 2020 to 2021 would have been 8.4%, as the economy continued to recover.
Despite worries that demand for telehealth could fall as the U.S. emerges from the COVID-19 pandemic, virtual care giant Teladoc beat Wall Street expectations with its 2021 financial results, and issued strong future growth projections Tuesday.
The New York-based vendor posted revenue of more than $2 billion in 2021, 86% higher than in 2020. Total visits were up 38% to 15.4 million, and Teladoc closed out the year with 53.6 million U.S. paid members, up just slightly from the year prior.
Beckers Hospital Review identifies 92 U.S. health systems with CMS-approved “hospital at home” programs.
Tired of grappling with the rising costs and poor quality of healthcare, a coalition of major healthcare purchasers is taking things into its own hands, establishing a company that is designing healthcare products to meet its members’ needs. “There’s an incredibly high frustration level among buyers of healthcare,” says Elizabeth Mitchell, president and CEO of the Purchaser Business Group on Health (PBGH) in San Francisco.
The nonprofit PBGH represents almost 40 large private employers and public entities that together spend $100 billion each year on healthcare services for more than 15 million Americans and their families. PBGH members include Microsoft, Walmart and American Airlines.
The decision to create the company, Emsana Health, was made about two years ago, with the initial focus on “really understanding the needs on a deep level,” Mitchell says. The company officially launched in the fall, and its first venture is setting up a pharmacy benefit manager (PBM), EmsanaRx, which went started operating on Jan. 1.
Finally, in a troubling tidbit, the Wall Street Journal reports
U.S. life insurers, as expected, made a large number of Covid-19 death-benefit payouts last year. More surprisingly, many saw a jump in other death claims, too.
Industry executives and actuaries believe many of these other fatalities are tied to delays in medical care as a result of lockdowns in 2020, and then, later, people’s fears of seeking out treatment and trouble lining up appointments.
Some insurers see continued high levels of these deaths for some time, even if Covid-19 deaths decline this year.
George Washington was born in Virginia on February 11, 1731, according to the then-used Julian calendar. In 1752, however, Britain and all its colonies adopted the Gregorian calendar which moved Washington’s birthday a year and 11 days to February 22, 1732.
Americans celebrated Washington’s Birthday long before Congress declared it a federal holiday. The centennial of his birth prompted festivities nationally and Congress established a Joint Committee to arrange for the occasion.
Washington’s Birthday was celebrated [as a federal holiday] on February 22nd [from 1879] until well into the 20th Century. However, in 1968 Congress passed the Monday Holiday Law to “provide uniform annual observances of certain legal public holidays on Mondays.” By creating more 3-day weekends, Congress hoped to “bring substantial benefits to both the spiritual and economic life of the Nation.”
One of the provisions of this act changed the observance of Washington’s Birthday from February 22nd to the third Monday in February. Ironically, this guaranteed that the holiday would never be celebrated on Washington’s actual birthday, as the third Monday in February cannot fall any later than February 21.
Contrary to popular belief, neither Congress nor the President has ever stipulated that the name of the holiday observed as Washington’s Birthday be changed to “President’s Day.”
Average daily COVID-19 cases and hospitalizations are continuing to fall in the U.S., providing a signal that the Omicron variant is receding across the country.
* * *
Deaths are also beginning to decline, with an average of about 2,100 daily, according to the data tracker from The New York Times. More than 2,500 daily deaths were being reported in early February.
The Omicron sublineage BA.2, which raised alarms because of its transmission advantage, accounts for just 4% of cases in the U.S., and experts suggested it’s not likely to reverse the current downward trend of cases overall.
BA.2 has certainly increased in prevalence, but its been a slow trajectory, according to CDC data. BA.1.1, another Omicron sublineage, actually became the dominant strain in the U.S. in mid-January, the agency reported, with the original lineage, B.1.1.529, currently accounting for about 23% of U.S. cases.
“The BA.2 Omicron variant is increasing in prevalence slowly in both CDC and private data,” tweeted Scott Gottlieb, MD, former FDA commissioner and current Pfizer board member. “While it may become a dominant strain in time, it appears increasingly unlikely that it will cause a significant change in the downward trajectory of the current epidemic wave.”
That has certainly been the case for South Africa, where BA.2 accounts for nearly 100% of cases, according to Tulio de Oliveira, PhD, of the Centre for Epidemic Response & Innovation in Stellenbosch.
“This comes on a background of decreasing infections,” de Oliveira tweeted. The country now has a 7-day average of about 2,500 daily infections, down from a peak of about 23,000 in mid-December.
“At present, the Omicron BA.2 is not of great concern in South Africa,” he tweeted. “But our network is following very close and is alerted to its emergence.”
From the Covid vaccination mandate front, the Society for Human Resource Management reports that the U.S. Court of Appeals for the Fifth Circuit ordered the lower court to reconsider whether United Airlines vaccination mandate offered sufficient protection under Tittle VII to religious objectors.
From the No Surprises Act front, the American Hospital Association tells us
The Centers for Medicare & Medicaid Services will host a conference call for health care providers Feb. 23 at 2 p.m. ET on the No Surprises Act’s continuity of care, provider directory and public disclosure requirements. To participate in the Special Open Door Forum, dial 888-455-1397 and reference passcode 5109694. Slides for the call are available here. Participants may email questions in advance to Provider_Enforcement@cms.hhs.gov. A recording will be available after the call through Feb. 25 by dialing 866-373-4993.
The cost of being transported by ground ambulance has increased steadily over the past five years, according to a new report from nonprofit Fair Health, threatening patients with few protections from balance billing in disputes between insurers and ambulance providers.
More ambulance trips are billing payers for advanced life support ( ALS), denoting a higher level of care (and reimbursement) than basic life support (BLS) services. Private insurers’ average payments for those trips increased 56% between 2017 and 2020, from $486 to $758, according to the analysis. Before accounting for discounts negotiated with payers, the rate that ambulance operators charged for trips jumped 23% in the same time period and now average almost $1,300.
However, the average reimbursement for advanced life support ambulance rides climbed by 5% for patients covered by Medicare, from $441 to $463, suggesting the government program is keeping a lid on rising costs.
Although at this point only air ambulance charges are subject to the No Surprises Act, this type of report could lead Congress to expand the law to include ground ambulance charges.
From the medical research front, Biopharma Dive informs us
Eli Lilly is again upping its investment in genetic medicine, announcing Tuesday plans to establish a Boston research center that will use RNA- and DNA-based technologies to develop new drugs.
The Lilly Institute for Genetic Medicine will take up 334,000 square feet in Boston’s Seaport neighborhood, with occupancy slated to begin in 2024. Lilly, which has earmarked around $700 million for the project, expects the institute to grow from 120 employees to 250 within five years. Roles will include data scientists, chemists and research biologists with expertise in genetic medicine.
Alongside drug development, the institute will take a page from another Lilly venture — Lilly Gateway Labs — and offer shared lab and office space to support biotechnology startups in the area. Use of the shared space, Lilly said, could create as many as 150 additional new jobs once it’s fully occupied.
Women who had ever experienced sexual violence in their lifetime — including sexual assault and workplace sexual harassment — were more likely to develop high blood pressure over a seven-year follow-up period, according to findings from a large, longitudinal study of women in the United States. The research, funded by the National Institutes of Health and published in the Journal of the American Heart Association, indicated that sexual violence was a common experience, affecting more than 20% of the women in the sample.
“Our results showed that women who reported experiencing both sexual assault and workplace sexual harassment had the highest risk of hypertension, suggesting potential compounding effects of multiple sexual violence exposures on women’s cardiovascular health,” said Rebecca B. Lawn, Ph.D.(link is external), of the Harvard T. H. Chan School of Public Health, Boston, lead author on the study.
From the healthcare initiative front, the Centers for Disease Control detailed its Million Hearts 2027 initiative.
From the virtual care front, Healthcare IT News tells us
The American Medical Association, in conjunction with Manatt Health, published a report this week exploring the ways that virtual care and other digital tools can accelerate the adoption of the integrated delivery of behavioral and physical healthcare.
In the report, the organizations note that behavioral health integration is essential for solving the country’s dire need for access to services.
“The demand for behavioral health services is significant and rising, but so is the potential for digital technology to support the integrated delivery of physical and behavioral health services,” said AMA President Dr. Gerald Harmon in a statement.
Moreover, in Health Affairs, the National Coordinator for Health Information Technology Micky Tripathi discusses delivering on the promise of health information technology in 2022.
From the healthcare business front, Healthcare Finance reports
The Department of Justice has until Saturday, February 27 to block the merger between UnitedHealth Group and Change Healthcare, according to a Securities and Exchange Commission filing on February 17.
The filing, by Change, was done in accordance with a timing agreement made with the DOJ. In November 2021, the two companies agreed not to consummate their merger before February 22.
The timing agreement provides the DOJ with 10 days’ notice to sue to block the deal.
“Effective February 17, 2022, UnitedHealth Group and the Company provided such notice to the DOJ,” Change said in the filing. “Accordingly, the DOJ now has until February 27, 2022 to initiate litigation to block the consummation of the merger.”
The DOJ is preparing the lawsuit to block UnitedHealth from purchasing Change, according to Seeking Alpha.
From the awards front
STAT News released its inaugural STATUS List which “recongizes standout individuals in health, medicine, and science. And although there are countless contenders to choose from, we’ve selected just 46 — an homage to the number of chromosomes in human DNA.”
OPM “announceda call for nominations for the 2022 Presidential Rank Awards (PRAs). A Presidential Rank Award is one of the most prestigious awards in the federal career civil service, and these awards are critical to recognizing the hard work and important contributions of dedicated civil servants in the American federal workforce. The awards – which recognize exceptional performance by members of the career Senior Executive Service (SES) and Senior Career Employees – reflect the Biden-Harris Administration’s commitment to supporting the federal workforce and recognizing federal employees who serve with distinction.” The nomination deadline is March 25, 2022.
We use cookies on our website to give you the most relevant experience by remembering your preferences and repeat visits. By clicking “Accept”, you consent to the use of ALL the cookies.
This website uses cookies to improve your experience while you navigate through the website. Out of these, the cookies that are categorized as necessary are stored on your browser as they are essential for the working of basic functionalities of the ...
Necessary cookies are absolutely essential for the website to function properly. These cookies ensure basic functionalities and security features of the website, anonymously.
Cookie
Duration
Description
cookielawinfo-checbox-analytics
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Analytics".
cookielawinfo-checbox-functional
11 months
The cookie is set by GDPR cookie consent to record the user consent for the cookies in the category "Functional".
cookielawinfo-checbox-others
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Other.
cookielawinfo-checkbox-necessary
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookies is used to store the user consent for the cookies in the category "Necessary".
cookielawinfo-checkbox-performance
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Performance".
viewed_cookie_policy
11 months
The cookie is set by the GDPR Cookie Consent plugin and is used to store whether or not user has consented to the use of cookies. It does not store any personal data.
Functional cookies help to perform certain functionalities like sharing the content of the website on social media platforms, collect feedbacks, and other third-party features.
Performance cookies are used to understand and analyze the key performance indexes of the website which helps in delivering a better user experience for the visitors.
Analytical cookies are used to understand how visitors interact with the website. These cookies help provide information on metrics the number of visitors, bounce rate, traffic source, etc.
Advertisement cookies are used to provide visitors with relevant ads and marketing campaigns. These cookies track visitors across websites and collect information to provide customized ads.