Mercer Marsh Benefits presents the top five trends from its 2023 employer-sponsored health plan survey of 225 insurers located in 56 countries:
Per-person medical cost increases are back to pre-pandemic levels. 68% of insurers expect plan sponsors to prioritize improvements. This is even though double-digit medical cost increases are forecast for some markets.
COVID-19 continues to impact the claims experience. 55% of insurers report an increase in the later-stage illness diagnosis due to deferred care.
Plan modernization has begun. To make coverage more inclusive for those who identify as LGBTQ+, one in two insurers have changed or expect to change eligibility requirements and eligible expenses.
The mental health gaps persist. 16% of insurers report not providing plans that cover mental health services (versus 26% in 2022).
Plan management requires greater rigor. More than one in five insurers in Asia are adjusting their medical plan premiums based on an individual’s COVID-19 vaccination status.
All five main points ring true, but the prime examples for the fourth and fifth points don’t fit the FEHB market.
The American Medical Association points out six often overlooked steps to better health while Rebecca G. Baker, Ph.D., the director of the NIH HEAL Initiative®looks back at a virtual stakeholder briefing to visit the initiative’s progress in resolving chronic pain and opioid misuse issues and to describe future plans.
From the public health front, the New York Times reports about
a large study published on Tuesday found a surprising trend among adolescents who repeatedly visited the hospital. The patients most likely to reappear in emergency rooms were not patients who harmed themselves, but rather those whose agitation and aggressive behavior proved too much for their caregivers to manage.
In many cases, repeat visitors had previously received sedatives or other drugs to restrain them when their behavior became disruptive. * * *
The results suggest that researchers should focus more attention on families whose children have cognitive and behavioral problems, and who may turn to emergency rooms for respite, Dr. [Anna] Cushing [an author of the study] said.
“I’m not sure we’ve been spending as much time talking about these agitated and behaviorally disregulated patients, at least on a national scale,” she said.
The JAMA study found that overall visits to pediatric emergency rooms for mental health crises increased 43 percent from 2015 to 2020, rising by 8 percent per year on average, with an increase in emergency visits for every category of mental illness. By comparison, emergency room visits for all medical causes rose by 1.5 percent annually.
Nearly one-third of visits were related to suicidal ideation or self-harm, and around one-quarter of patients presented with mood disorders, followed by anxiety disorders and impulse control disorders. Around 13 percent of patients made a repeat visit within six months.
There are few things more stressful than getting a serious medical diagnosis, but pandemic-era changes in virtual care are prompting more patients to obtain a second opinion without leaving home.
Why it matters: The telehealth explosion made it easier to get advice from top doctors across the country — and for health systems to grow business beyond their physical footprints and even treat some of the people seeking consultations.
Case in point: The Clinic, a joint venture between Cleveland Clinic and telehealth giant Amwell, launched in 2020 just before the pandemic began.
The idea was to pair the Cleveland Clinic brand with Amwell’s virtual tools and its existing connections with private insurers to make it easier for patients to get their records reviewed, said Frank McGillin, CEO of The Clinic.
In litigation news, Health Payer Intelligence relates
A United States district court has ruled against Blue Cross Blue Shield of Illinois (BCBSIL), stating that the payer cannot exclude coverage for medically necessary gender-affirming care in its employer-sponsored ERISA health plans.
Lambda Legal and Sirianni Youtz Spoonemore Hamburger PLLC filed a class action lawsuit against BCBSIL on behalf of a 17-year-old transgender man, CP, and his parents. According to the lawsuit, the payer administered discriminatory exclusions of gender-affirming care, violating the anti-discrimination of the Affordable Care Act (ACA), known as Section 1557. * * *
The court determined that BCBSIL is a “health program or activity” that receives federal funds and thus cannot discriminate based on race, national origin, sex, age, or disability in its role in administering ERISA health plans.
From Capitol Hill, the National Rural Healthcare Association trumpets the “big rural health advocacy wins in FY23 appropriations bill” that the President will be signing this week. Notably —
Given the devastating outcome of COVID-19 in rural areas, NRHA has been committed to working with Capitol Hill to see an Office of Rural Health created at the Centers for Disease Control and Prevention (CDC). Included in the FY 2023 appropriations bill was $5 million to establish an Office of Rural Health at CDC. The text dictates that the ORH will enhance implementation of CDC’s rural health portfolio, coordinate efforts across CDC programs, and develop a strategic plan for rural health that maps the way forward both administratively and programmatically. This is a massive victory for rural health, and NRHA is looking forward to working with CDC to see this stood up quickly, to ensure rural representation in America’s public health infrastructure.
$3.45 billion for the Rural Community Facilities Program and $2 million for the Rural Hospital Technical Assistance Program through the United States Department of Agriculture Rural Development (RD) programs.
Omicron subvariant XBB is encroaching on BQ.1 and BQ.1.1’s dominance, CDC data shows, as it accounts for 18.3 percent of U.S. cases and makes up more than 1 in 2 infections in the Northeast.
Subvariants BQ.1 and BQ.1.1, which became the nation’s most pervasive strains in November, are on the decline.
The FDA began tracking XBB on Nov. 28. The subvariant is a fusion of two other omicron subvariants, BA.2.10.1 and BA.2.75, and it caused a wave of cases in Singapore. Eric Topol, MD, founder and director of Scripps Research Translational Institute in San Diego, wrote Dec. 23 that XBB mutation XBB.1.5 “has the most growth advantage vs. BA.5,” which was causing most COVID-19 cases for months.
Beckers also reports, “The CDC issued a health advisory on Dec. 22 to alert the medical community of a rise in severe strep A infections among children. * * * Read the full advisory and provider recommendations here.”
From the U.S. healthcare business front, the Wall Street Journal challenges non-profit hospital business practices which fail to help the needy.
Many of the nation’s largest nonprofit hospital systems, which give aid to poorer communities to earn tax breaks, have been leaving those areas and moving into wealthier ones as they have added and shed hospitals in the last two decades.
As nonprofits, these regional and national giants reap $8.8 billion from tax breaks annually, by one Johns Hopkins University researcher’s estimate. Among their obligations, they are expected to provide free medical care to those least able to afford it.
Many top nonprofits, however, avoid communities where more people are likely to need that aid, according to a Wall Street Journal analysis of nearly 470 transactions. As these systems grew, many were more likely to divest or close hospitals in low-income communities than to add them. * * *
Ascension was the most active deal maker in the Journal’s review. Through deals involving 93 hospitals over the past 20 years, Ascension has grown into one of the largest U.S. systems, with $28 billion in revenue and $19.5 billion in cash reserves in its most recent fiscal year, ended June 30.
Among the hospitals Ascension pruned as it grew were those serving some of the poorest neighborhoods of Washington, D.C., and Chicago.
Local elected officials said that when a system exits a market, it can be difficult for remaining facilities to serve the community.
The Journal also questions online advertising for prescription drugs by certain telehealth companies.
In an advertisement on Facebook and Instagram, a middle-aged man holding a dumbbell says testosterone “literally changed my life,” restoring his energy and happiness.
What the October ad from telehealth startup Hone Health doesn’t say is that the unidentified man is an actor who has never used the prescription drug. It doesn’t mention that testosterone is approved by the Food and Drug Administration only for men with specific disorders and that among its risks are heart attacks and stroke.
Similar telehealth companies are flooding TikTok, Instagram and other platforms with ads that don’t conform to longtime standards governing the marketing of prescription drugs and healthcare treatments. They feature actors posing as customers, tout benefits of drugs with no mention of side effects and promote medications for uses not approved by the FDA.
In the two years since the government expanded the scope of medical services allowed via video calls, telehealth companies have been operating largely outside advertising rules that govern drugmakers, a gray area subject to little government oversight or guidance. Instead, the main gatekeepers exercising the power to review or remove telehealth advertising are the social-media giants paid to run the ads.
From Capitol Hill, the American Hospital Association tells us
The Senate today passed (68-29) an amended version of the $1.7 trillion omnibus appropriations bill that funds the federal government through the end of the current fiscal year. The legislation also includes many provisions affecting hospitals and health systems.
The Senate also passed another short-term continuing resolution through Dec. 30 to allow time for the more than 4,000-page legislation to be enrolled and for President Biden to sign it. This ensures there will be no interruption of services or federal shutdown.
The omnibus spending bill, which includes relief from Medicare cuts and extensions of rural and telehealth programs, as well as the Dec. 30 continuing resolution, now go to the House, which is expected to consider them today . The president is expected to sign the short-term continuing resolution before current funding for the government expires at 11:59 p.m. ET on Dec. 23, and to sign the omnibus later next week.
The Wall Street Journal adds, “House Majority Leader Steny Hoyer (D., Md.) said the House would vote on the bill Friday.”
In other 2023 Consolidated Appropriations Act or omnibus news
The Hill reports on “last minute” changes to the omnibus, including provisions assisting nursing and pregnant workers.
Mercer Consulting alerts us to a two-year-long extension of telehealth flexibilities available to high deductible plans with health savings accounts.
Think Advisor and the Wall Street Journal provide an overview of the Secure 2.0 Act provisions in the omnibus. The Secure 2.0 Act affects 401(k) plans offered to employees and IRAs. The key provision that takes effect for 2023 is an increase in the required minimum distribution age from 72 to 73.
The Wall Street Journal reviews the other omnibus provisions affecting businesses.
While the respiratory “tripledemic” continues to slam emergency rooms and children’s hospitals, there are two glimmers of hope on the horizon, according to a Dec. 22 report in The New York Times.
COVID-19, the flu and respiratory syncytial virus attack the body in different ways, and there are varying levels of disease severity across the U.S. Today, some scientists say RSV has peaked in most parts of the country.
“I think it’s likely that the RSV season has peaked in most parts of the country,” said Virginia Pitzer, ScD, an infectious disease epidemiologist at New Haven, Conn.-based Yale School of Public Health. “I think that there is a light at the end of the tunnel.”
Additionally, there’s reason to believe next winter won’t be as burdensome for the American population and healthcare organizations.
Ironically, the safety precautions used to help stem the pandemic in the past couple of years have also kept adults and children from being exposed to the viruses that typically circulate this time of year, said Dr. Pitzer.
“There was a bit of a buildup of susceptibility at the population level,” she added. “It’s a worse than normal winter, but one that hopefully will not be repeated next year.”STS
The Society for Healthcare Epidemiology of America today recommended hospitals and health systems no longer routinely screen symptom-free patients for COVID-19 upon admission or before procedures and rely instead on enhanced layers of infection prevention interventions.
“The small benefits that could come from asymptomatic testing at this stage in the pandemic are overridden by potential harms from delays in procedures, delays in patient transfers, and strains on laboratory capacity and personnel,” said Thomas R. Talbot, M.D., MPH, the chief hospital epidemiologist at Vanderbilt University Medical Center, and a member of the SHEA Board of Directors. “Since some tests can detect residual virus for a long period, patients who test positive may not be contagious.”
[According to a CDC report, a] baby born in the U.S. in 2021 has a life expectancy of 76.4 years, down from 77 years in 2020 and the lowest level the CDC has recorded since 1996. The age-adjusted death rate for Covid rose by 22.5% between 2020 and 2021, while death rates from unintentional injuries — one-third of which come from overdoses — rose by 12.3%.
HHS’s Agency for Healthcare Quality and Researched refreshed its Healthcare Cost and Utilization Project Fast Stats website. The site provides “summary statistics on inpatient stays, emergency department visits, and priority topics, by select characteristics.”
From the OPM front, OPM’s medical director, Dr. Ron Kline announced today on Linked In that he is leaving OPM to take a new position beginning January 17, 2023 as
the Chief Medical Officer of the Quality Measurement and Value-Based Incentives Group (QMVIG) at the Center for Clinical Standards and Quality (CCSQ) at the Centers for Medicare & Medicaid Services (CMS).
QMVIG is responsible for developing, evaluating and supporting the implementation of quality measurement programs across the entire federally-supported health care continuum. This includes Medicare’s Quality Payment Program and the Inpatient (i.e. Hospital) Quality Reporting Program. These measures and policies guide these innovative programs to improve healthcare quality for all Americans.
Best wishes, Dr. Kline, and thanks for your work with the FEHB over the past 3 1/2 years.
From the Rx coverage and medical research fronts –
The Food and Drug Administration (FDA) has approved Actemra (tocilizumab) for intravenous (IV) use to treat COVID-19 in hospitalized adults who are receiving systemic corticosteroids and require supplemental oxygen, noninvasive or invasive mechanical ventilation or extracorporeal membrane oxygenation (ECMO).
The latest Alzheimer’s disease treatment from Eisai and Biogen needs to be cheaper than $20,000 a year to be cost-effective, according to a draft analysis from an influential nonprofit organization published Thursday.
The Institute for Clinical and Economic Review, or ICER, dug into the evidence for lecanemab and concluded that the drug’s demonstrated benefits, a modest but statistically significant delay in the advance of Alzheimer’s, are worth between $8,500 and $20,600 per year. ICER’s calculations, which could change in response to public comment over the next month, are based on metrics meant to quantify the value of improvements to quality of life.
Eisai, which is leading the effort to commercialize lecanemab, has not disclosed how much it will charge for the medicine, saying only that it will prize affordability and access. That will soon change, as the drug, a twice-monthly infusion, is expected to win a preliminary Food and Drug Administration approval by Jan. 6. * * *
Lecanemab’s safety has come into sharp focus over the past two months after three patients died of major brain bleeds.
The Institute for Clinical and Economic Review (ICER) today released a Final Evidence Report assessing the comparative clinical effectiveness and value of etranacogene dezaparvovec (Hemgenix, CSL Behring,) for hemophilia B. ICER also updated the previous Hemophilia A assessment on valoctocogene roxaparvovec (Roctavian™, BioMarin).
Key recommendations stemming from the roundtable discussion include:
The value of high-impact single and short-term therapies should not be determined exclusively by estimates of long-term cost offsets, particularly when the existing standard of care is acknowledged to be priced significantly higher than reasonable cost-effective levels.
Payers should work with manufacturers to develop and implement outcomes-based agreements to address the uncertainty and the high cost of gene therapies for hemophilia.
At least one national payer has suggested to patient representatives that step therapy with emicizumab is being considered prior to provision of coverage for Roctavian. Clinical experts and patient experts view this approach as lacking any clinical justification and appears to be only a method for trying to avoid the high one-time fee for gene therapy while assuming that patients may switch insurers before the cost-saving potential of gene therapy is fully realized. In short, step therapy does not appear to be a reasonable consideration for this treatment.
ICER’s detailed set of policy recommendations, including comprehensive considerations for establishing evidence-based prior authorization criteria, is available in the Final Evidence Report and in the standalone Policy Recommendations document.
Scientists used patient stem cells and 3D bioprinting to produce eye tissue that will advance understanding of the mechanisms of blinding diseases. The research team from the National Eye Institute (NEI), part of the National Institutes of Health, printed a combination of cells that form the outer blood-retina barrier—eye tissue that supports the retina’s light-sensing photoreceptors. The technique provides a theoretically unlimited supply of patient-derived tissue to study degenerative retinal diseases such as age-related macular degeneration (AMD).
If you haven’t yet tried ChatGPT, OpenAI’s new artificial-intelligence chatbot, it will blow your mind. Tell the bot to write you anything—an email apologizing to your boss, an article about the world’s richest hamster, a “Seinfeld” script set in 2022—and it spits out text you’d think was written by a human. Knowledge of the topic, proper punctuation, varied sentence structure, clear organization. It’s all there.
From the Centers for Disease Control’s Covid data tracker and its weekly interpretative summary of its Covid statistics:
New Cases totaled 455.556 this week, down 2.7% from last week.
Variants BQ.1.1 and BQ.1 are estimated to represent 78% of Covid / Omicron cases
New Hospitalizations averaged 5,010 this week, up 2.3% from last week.
New Deaths totaled 2,703, down 13.2% from last week.
“As of December 14, 2022, 660.4 million vaccine doses have been administered in the United States. About 228.8 million people, or 68.9% of the U.S. population, have completed a primary series.* More than 44.2 million people, or 14.1% of the U.S. population ages 5 years and older, have received an updated (bivalent) booster dose.”
The CDC reports good news about the efficacy of the bivalent booster here and here.
Pfizer announced the sale $2 billion worth of Paxlovid pills (3.7 million courses) to the federal government and its ongoing research on developing combined mRNA Covid and flu vaccine.
From CDC’s Fluview — “Seasonal influenza activity remains high but appears to be declining in some areas.”
Leaders at hospitals and health systems across the country are anticipating a potentially turbulent operating environment in the coming year, according to a survey from Deloitte.
Among health system leaders, 85% said staffing challenges would have a major impact on their 2023 strategy and 76% said inflation is a significant factor. Other expected headwinds include affordability issues for patients, shrinking margins and continual supply chain disruptions.
Deloitte also polled health plan executives and found they face challenges related to inflation and a tight labor market, though are generally in a better financial position than hospitals and health systems.
Speaking of hospitals, Fierce Healthcare informs us
The care given in emergency departments came under fire yesterday with the release of a government study saying that 250,000 Americans die every year due to misdiagnoses.
The findings spurred an immediate response from the president of the American College of Emergency Physicians (ACEP), who questions the study’s veracity and methodology.
Christopher S. Kang, M.D., president of the ACEP, said in a statement that “in addition to making misleading, incomplete and erroneous conclusions from the literature reviewed, the report conveys a tone that inaccurately characterizes and unnecessarily disparages the practice of emergency medicine in the United States.”
One of the authors of the study—David Newman-Toker, M.D., Ph.D., a neurologist at Johns Hopkins University—vehemently defends the methodology and told Fierce Healthcare that “high levels of variation in care (across conditions, across hospitals, across demographic groups) tells us that these errors do not need to be thought of as ‘the price of doing business.’ It tells us that there are already probably ways to get it right.”
The study, conducted by Johns Hopkins for the Agency for Healthcare Research and Quality, states that among 130 million ED visits in the U.S. per year, 7.4 million patients are misdiagnosed. In addition, 2.6 million suffer an adverse event, and about 370,000 suffer serious harm from diagnostic errors.
The teenage daughter of CNN reporter Jake Tapper writes in CNN about her frightening ER experience. The FEHBlog joined his wife at a Dripping Springs TX knitting store holiday event. He mentioned the Alice Tapper story to two nurses who were horrified. In the FEHBlog experience, nurses are the best judge of hospital care across facilities.
In HIPAA news, the American Hospital Association tells us
The Department of Health and Human Services yesterday proposed a standard format for attachments to support electronic health care claims and prior authorization transactions under the Health Insurance Portability and Accountability Act. The standard would apply to all health plans, health care clearinghouses, and providers, who currently lack an efficient and uniform method of sending attachments, which can lead to provider burnout, slow down processing and delay payments or patient care.
“The AHA supports establishing a standard for attachments to reduce the administrative burdens facing clinicians, and we look forward to providing robust commentary after analyzing the rule’s specifics,” said Terrence Cunningham, AHA’s director of administrative simplification policy.
From Capitol Hill, the Wall Street Journal reports
The House on Wednesday passed a one-week government funding measure to give congressional negotiators time to complete and pass a full-year omnibus spending bill, overcoming opposition from Republicans who urged postponing any deal until next year, when the GOP will take control of the chamber. * * *
The Senate is expected to next approve the one-week extension [on Thursday December 15].
The vote on a one-week continuing resolution, which keeps the government funded at fiscal 2022 spending levels, follows the announcement Tuesday that Democratic and Republican negotiators had reached agreement on a framework and would turn to completing the details.
From the public health front, Healthcare Dive tells us
National health spending grew almost 3% in 2021, reaching $4.3 trillion as big increases in healthcare use and insurance coverage were offset by lower government spending on COVID-19.
The year’s growth rate was smaller than the 10% notched in 2020. CMS actuaries chalked the deceleration up to lower federal health spending, which fell 3.5% in 2021 compared to a 37% increase in 2020 as funding to combat the pandemic skyrocketed.
Health spending grew at a much slower clip than the nation’s gross domestic product, which increased 11% in 2021 — the largest growth rate since 1984.
Here’s the report which is posted on Health Affairs.
New more aggressive targets for blood pressure and lipids are among the changes to the annual American Diabetes Association (ADA) Standards of Care in Diabetes — 2023.
The document, long considered the gold standard for care of the more than 100 million Americans living with diabetes and prediabetes, was published December 12 as a supplement in Diabetes Care. The guidelines are also accessible to doctors via an app; last year’s standards were accessed more than 4 million times.
The Agency for Healthcare Quality and Research’s Director is posting a series of four reports concerning the agency’s effort to rethink healthcare quality in view of the fact
In seven years, the United States is expected to reach a demographic tipping point that will redraw the picture of healthcare delivery in America.
In 2030, all baby boomers [birth dates from 1946 to 1964] will be older than 65, according to the U.S. Census Bureau. Just four years later—in 2034—older adults will outnumber children for the first time in history. The scope of this and future demographic shifts—including our population’s growing racial and ethnic diversity—will profoundly impact how healthcare is accessed, delivered, paid for, and evaluated.
The National Institutes of Health reports “Two randomized, placebo-controlled trials evaluating three Ebola vaccine administration strategies in adults and children found that all the regimens were safe in both age groups, according to results published today in the New England Journal of Medicine.”
Privately-insured Americans experienced higher rates of heat-related illness diagnoses in 2021 compared to 2016, in some cases a more than 37 percent increase, according to a report from FAIR Health.
“The Centers for Disease Control and Prevention has identified projected increases in extreme summer heat as one source of adverse health impacts from climate change. However, systematic, national data on trends in heat-related illnesses in the United States have been lacking,” the report began.
From the omicron and siblings front, a subset of public health —
The New York Times explores the question — who are the never Coviders? Even if you have never had Covid, you certainly have been impacted mightily by Covid. Nevertheless, it is an interesting article.
MedPage Today notes “Long COVID played a role in more than 3,500 deaths in the U.S. since the start of the pandemic, according to data from the CDC’s National Center for Health Statistics (NCHS).” The NCHS report may be overestimating because the first death occurred in April 2020 just after Covid got rolling and the most commonly mentioned term on death certificates with long COVID was “post COVID,” which was mentioned in 89.6% of long COVID-related deaths.” This may be a rare case in which the “retrospectoscope” is cloudy. See Dr. Martin Markary’s opinion piece on long Covid in yesterday’s Wall Street Journal.
From the regulatory front —
CMS issued a proposed rule on Medicare Part D changes for 2024.
Health Affairs began a series of three informative articles on the proposed 2024 notice of benefit payments and parameters released on Monday.
STAT News discusses a feature of the parameters notice that is drawing industry attention. To wit, “The Biden administration signaled Monday that it will require health plans on federal exchanges to cover more of the costs of generic drugs, a small tweak that nevertheless has industry groups divided on how best to manage drug costs.”
Health Leaders Media examines the gap that must be bridged to achieve a recent HHS proposed rule’s goal of implementing electronic prior authorization.
In agency event news —
OPM issued a press release about its “first government-wide summit for diversity, equity, inclusion, and accessibility (DEIA) on December 6-8, 2022.”
Federal News Network reports on the Office of Management and Budget’s event celebrating and reflecting on the first anniversary of the President’s Management Agenda.
Top appropriators struck a deal Tuesday night on a government funding framework critical to finalizing a mammoth year-end spending package.
In a statement, retiring Senate Appropriations Chair Patrick Leahy (D-Vt.) said appropriators have “reached a bipartisan, bicameral framework that should allow us to finish an omnibus appropriations bill that can pass the House and Senate and be signed into law by the President.”
Leading negotiators didn’t release those government funding totals in announcing the deal, but appropriators have largely settled on an $858 billion defense budget in recent weeks.
That’s good news. Presumably, Congress still plans to extend the continuing resolution from December 16 to December 23 this week in order to allow time to write and pass the omnibus bill.
From the Omicron and siblings front, Healthcare Dive reports that
In the two years since the COVID-19 vaccine became available for U.S. patients, the country’s vaccination program prevented more than 18.5 million hospitalizations and 3.2 million deaths, according to new research from the Commonwealth Fund and Yale School of Public Health.
Many millions of infections were prevented, preserving hospital resources for patients who otherwise would not have received timely care, the researchers said. The vaccine also saved the country $1.15 trillion in medical costs, kept children in school and allowed businesses to reopen, the study said.
To arrive at its findings, the study used a computer model of disease transmission, comparing the pandemic trajectory to a simulated scenario without a vaccination program. The results can be used to inform future evidence-based decisions on vaccine use to reduce disease burden, the researchers said.
The FEHBlog has no doubt that the rapidly developed mRNA vaccines pulled us out of a jam in winter 2020 while Paxlovid and other anti-virals saved us from the monstrous Omicron surge in winter 2021.
From the CMS front —
CMS has activated the Ground Ambulance and Patient Billing Advisory Committee required by the No Surprises Act. The Committee’s report likely will be released in the second quarter of 2023.
CMS released a readout from “We Can Do Better: Advancing Maternity Care Together – the first CMS convening on maternal health since the agency launched its Maternity Care Action plan in July 2022 as part of the Biden-Harris Administration’s Blueprint for Addressing the Maternal Health Crisis. Attendees discussed key actions to improve the health of pregnant and postpartum individuals – including the need for a robust and diverse maternity care workforce and the ability for consumers to easily identify health systems engaged in improving maternal care.”
CMS also called attention to the “recently released proposed rule that, if finalized, would modify the current National Council for Prescription Drug Programs (NCPDP) retail pharmacy standards for electronic transactions and expand the applicability of the Medicaid pharmacy subrogation transaction to all health plans.”
In related news, EHR Intelligence tells us, “In a recent letter, Health Level Seven International (HL7) called on the National Committee on Vital and Health Statistics (NCVHS) to include FHIR as a data standard for electronic clinical attachments. NSG encourages the public to submit comments on the proposed rule by January 9th, 2023.” The original version of HIPAA enacted over 25 years ago called for this attachments standard, which has been a thorn in CMS’s side.
In other HHS news —
HHS’s Agency for Healthcare Quality and Research informs us that the U.S. Preventive Services Task Force has proposed to keep in place the grade A recommendation “that clinicians prescribe pre-exposure prophylaxis with effective antiretroviral therapy to persons who are at increased risk of HIV acquisition to decrease the risk of acquiring HIV infection.” The original PREP recommendation was made in 2018.
The American Hospital Association relates “The Substance Abuse and Mental Health Services Administration today proposed updating opioid treatment program standards and admission criteria to expand access to treatment. According to the agency, the rule would expand the definition of OTP practitioner to include any provider appropriately licensed to dispense and/or prescribe approved medications; no longer require one year of opioid addiction for admission; add evidence-based delivery models such as telehealth; expand patient access to take-home methadone doses, and no longer require annual reports from practitioners with a waiver to prescribe buprenorphine to up to 275 patients. The agency will accept comments on the proposed rule through Feb. 14.” That makes sense to the FEHBlog.
From the drug development front —
The Wall Street Journal reports
A customized Moderna Inc. MRNA 19.63%increase; green up pointing triangle vaccine helped ward off the recurrence of melanoma in a mid-stage trial, a milestone in long-running efforts to use the shots as treatments and a big step in the biotech’s ascent.
The combination of Moderna’s personalized cancer vaccine and MerckMRK 1.78%increase; green up pointing triangle & Co.’s Keytruda cancer immunotherapy reduced patients’ risk of relapse or death by about 44%, versus Keytruda alone, in the 150-volunteer study, the companies said Tuesday.
The results, which the companies said were statistically significant but haven’t been reviewed by independent scientists, suggest promise for an emerging but unproven class of vaccines that aim to treat diseases rather than prevent infections like typical shots.
Multiple myeloma can be treated by several drugs but relapse in this type of blood cancer is common and when that happens, patients need other treatment options. Johnson & Johnson is looking to fill that need with a drug that addresses a novel target. The pharmaceutical company is seeking regulatory approval for this molecule and the most up to date clinical data supporting the application were presented during the annual meeting of the American Society of Hematology (ASH).
Patients in the Phase 1/2 clinical trial had some of the toughest cases that progressed after treatment with at least three different therapies, according to Ajai Chari, director of clinical research in the multiple myeloma program at Mount Sinai and an investigator in the study. Despite that, treatment with the J&J drug, talquetamab, led to response rates of up to 74%.
From the healthcare business front, Fierce Healthcare tells us
Operating margins for the three largest for-profit hospital chains exceeded pre-pandemic levels in the third quarter, according to a new analysis that comes as hospital lobbies are pushing for financial relief from Congress.
The analysis, released Monday by the Kaiser Family Foundation, looked at the latest financial performance for large hospital chains HCA Healthcare, Tenet Healthcare and Community Health Systems. * * *
Kaiser’s analysis comes a day after The Wall Street Journal published a report that showed hospitals received billions of dollars in aid, with some going to profitable systems that didn’t need it. Part of the problem was a mismatch in the federal government’s allocation of the $175 billion Provider Relief Fund passed by Congress at the onset of the pandemic in early 2020, the report said.
From the tidbits department, the FEHBlog learned at the ABA Washington Health Law Summit today
The third Texas Medical Association case filed November 30 and pending before District Judge Kernodle concerns the manner in which the qualifying payment amount is calculated – a new issue which nevertheless could have been joined to the second lawsuit. Go figure.
In 2018, Congress passed a law called the Eliminating Kickbacks in Recovery Act (“EKRA”), 18 U.S.C. § 220. The Epstein, Becker and Green law firm explains, “EKRA initially targeted patient brokering and kickback schemes within the addiction treatment and recovery spaces. However, since EKRA was expansively drafted to also apply to clinical laboratories (it applies to improper referrals for any “service”, regardless of the payor), public as well as private insurance plans and even self-pay patients fall within the reach of the statute.”
Based on the Centers for Disease Control’s Covid Data Tracker, the CDC’s weekly interpretation of those new cases, hospitalizations and death statistics shows across-the-board increases. Welcome winter.
New Cases
As of December 7, 2022, the current 7-day average of weekly new cases (65,569) increased 49.6% compared with the previous 7-day average (43,825). A total of 99,241,649 COVID-19 cases have been reported in the United States as of December 7, 2022.
Variant Proportions
CDC Nowcast projections* for the week ending December 10, 2022, estimate the proportion of lineages designated as Omicron with estimates above 1%: BA.5—and four of its sublineages (BQ.1, BQ.1.1, BF.7, and BA.5.2.6)—BA.4.6, and XBB. XBB is a recombinant of two BA.2 sublineages.
The two predominant Omicron lineages and the two that are increasing this week are BQ.1.1, projected to be 36.8% (95% PI 34.1-39.6%) and BQ.1, projected to be 31.1% (95% PI 29.0-33.4%) nationally. All other lineages (BA.5, BF.7, XBB, BN.1, BA.5.2.6, and BA.4.6) are decreasing in proportion this week compared to last.
New Hospitalizations
The current 7-day daily average for November 30–December 6, 2022, was 4,844. This is a 13.8% increase from the prior 7-day average (4,256) from November 23–29, 2022.
New Deaths
The current 7-day average of new deaths (426) increased 61.7% compared with the previous 7-day average (263). As of December 7, 2022, a total of 1,080,472 COVID-19 deaths have been reported in the United States.
Hospitals are more full than they’ve been throughout the Covid-19 pandemic, according to a CNN analysis of data from the US Department of Health and Human Services. But as respiratory virus season surges across the US, it’s much more than Covid that’s filling beds this year.
More than 80% of hospital beds are in use nationwide, jumping 8 percentage points in the past two weeks.
Hospitals have been more than 70% full for the vast majority of that time. But they’ve been 80% full at only one other point: in January, during the height of the Omicron surge in the US. Back in January, about a quarter of hospital beds were in use for Covid-19 patients. But now, only about 6% of beds are in use for Covid-19 patients, according to the HHS data.
From the Omicron countermeasures front, the weekly interpretation tells us
As of December 7, 2022, 657.9 million vaccine doses have been administered in the United States. Overall, about 228.6 million people, or 68.9% of the total U.S. population, have completed a primary series.* More than 42.0 million people, or 13.5% of the U.S. population ages 5 years and older, have received an updated (bivalent) booster dose.
Medscape adds, “Getting at least one dose of a COVID-19 vaccine decreases the chances of having symptoms beyond 3 weeks or developing long COVID, a new analysis shows.”
The weekly interpretation usually encourages more Covid vaccinations. This week, the interpretation opens by touting the use of Paxlovid, to wit —
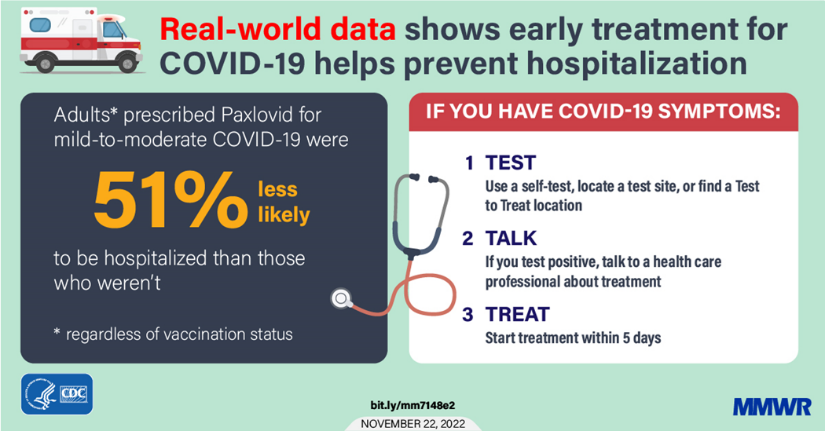
As we enter the holiday season, it’s important to take steps to protect yourself and others from serious illness with COVID-19, including staying up to date on COVID-19 vaccines and promptly talking to your healthcare provider about treatment options if you test positive for COVID-19.
If you have COVID-19 symptoms:
Test : Use a self-test, locate a test site, or find a Test to Treat location.
Talk: If you test positive, talk to a healthcare professional to determine if you are eligible for treatment, even if your symptoms are mild right now.
Treat: Start treatment within five days of developing symptoms.
Note to Readers: Paxlovid is not a replacement for COVID-19 vaccination. COVID-19 vaccination makes you much less likely to get very sick. Still, some vaccinated people, especially those ages 65 years or older or who have other risk factors for severe disease, may benefit from treatment if they get COVID-19. A healthcare provider will help decide which treatment, if any, is right for you.
That’s the full picture for most folks. Here’s the “real-world data” link if you are interested. Thank you CDC.
Here are the key points from this week’s CDC FluView:
Seasonal influenza activity is high across the country.
Of the influenza A viruses detected and subtyped during week 48, 76% have been influenza A(H3N2), and 24% have been influenza A (H1N1).
Seven influenza-associated pediatric deaths were reported this week, for a total of 21 pediatric flu deaths reported so far this season.
CDC estimates that, so far this season, there have been at least 13 million illnesses, 120,000 hospitalizations, and 7,300 deaths from flu.
The cumulative hospitalization rate in the FluSurv-NET system is higher than the rate observed in week 48 during every previous season since 2010-2011.
The number of flu hospital admissions reported in the HHS Protect system increased during week 48 compared to week 47.
The majority of influenza viruses tested are in the same genetic subclade as and antigenically similar to the influenza viruses included in this season’s influenza vaccine.
All viruses collected and evaluated this season have been susceptible to influenza antivirals.
An annual flu vaccine is the best way to protect against the flu. Vaccination helps prevent infection and can also prevent serious outcomes in people who get vaccinated but still get sick with the flu.
CDC recommends that everyone ages 6 months and older get a flu vaccine annually. Now is a good time to get vaccinated if you haven’t already.
There are also prescription flu antiviral drugs that can be used to treat flu illnesses. It’s very important that flu antiviral drugs are started as soon as possible to treat patients who are hospitalized with flu, people who are very sick with flu but who do not need to be hospitalized, and people with flu who are at higher risk of serious flu complications based on their age or health.
Multiple respiratory viruses are currently co-circulating with influenza. Testing is important to determine the appropriate treatment.
From the FEHB front, the FEHBlog was bowled over to discover on reginfo.gov that on November 29, the Office of Personnel Management took a major step forward in implementing the Postal Service Health Benefits Program by submitting a draft interim final rule to OMB’s Office of Information and Regulatory Affairs for its review. This is the final step before the rule is published in the Federal Register. The statutory deadline for so promulgating this rule is April 8, 2023.
From the miscellany department
HR Dive discusses a Mercer report on how employers can impact the maternal mortality problem.
EBRI offers a useful analysis of telemedicine and its relationship with other healthcare services, enrollee health, and costs.
Chain Drug News reports that PCMA, the prescription drug manager trade association, has issued policy recommendations to accelerate patient biosimilar drug use.
The Wall Street Journal offers encouraging news about prison programs to resolve inmate addiction issues.
Two-thirds of people entering prisons and jails have what the Department of Health and Human Services diagnoses as substance-use disorder. For years, the only treatment in all but a handful of detention centers was to detox.
Some 630 of the roughly 5,000 jails and prisons nationwide now provide medication treatment for opioid use, according to the nonprofit Jail and Prison Opioid Project, up from about 20 in 2015. The drugs include buprenorphine, which tamps cravings for opioids, naloxone, which reverses their effects, and methadone, which eases withdrawal symptoms. Some are taken daily, others can be taken once a month in extended-release versions. The Biden administration said it wants medication available for every drug user in federal custody and at half of state prisons and jails by 2025.
From Capitol Hill, the Wall Street Journal reports
Senate Democrats celebrated their win in Georgia giving them 51 seats next year, a result that enhances their power by allowing them to more easily advance President Biden’s nominees while also providing slightly more flexibility on legislation.
Sen. Raphael Warnock’s win in a runoff election over GOP challenger Herschel Walker comes after two years in which Vice President Kamala Harris provided a tiebreaking vote in the 50-50 Senate. * * *
Since early 2021, the two parties have been operating under a power-sharing agreement with evenly divided committees, which has prevented Democrats from issuing subpoenas to witnesses without GOP support. When nominees have tied in a committee vote, Democrats have been forced to hold an extra procedural vote to finalize their nomination. The Warnock victory will give Democrats a narrow majority on each panel.
“It’ll be easier for Democrats to move forward with some of their nominees, particularly in the judiciary, and that makes it more difficult for us,” said Sen. Mitt Romney (R., Utah).
The newly minted defense authorization bill for fiscal 2023 [NDAA], made public Tuesday night, provides a shot in the arm to the U.S. defense budget but bars the military from discharging any more troops who refuse COVID-19 vaccine shots in their arms. * * *
[This bill has been approved by a House-Senate conference committee.] The House is expected to vote on the NDAA as soon as Thursday and the Senate to soon follow suit, perhaps next week.
The bill would authorize a 4.6 percent across the board pay increase for military personnel and civilians. However, House and Senate negotiators removed a House-passed “inflation bonus” of an additional 2.4 percent for troops and Defense Department civilians making less than $45,000 a year. * * *
Also of note, the bill would ban contractors across the government from using Chinese-made semiconductors, after a lengthy phase-in period, an aide with knowledge of the provision said Tuesday. Many federal contractors and other businesses say they are unclear how they will comply.
Govexec offers two more insights on the NDAA
Congressional negotiators on Tuesday night finally revealed a compromise version of the annual defense policy bill with the aim of passing it through both the House and Senate this week. But to some lawmakers, federal employee groups and good government experts’ chagrin, the measure did not include [Insight link] a provision aimed at blocking Republican-led efforts to strip potentially tens of thousands of federal employees of their civil service protections.
and
The authorization bill compromise text contains provisions [Insight link] that seek to increase transparency and accountability of investigations into Inspectors Generals [IG] and operations of the Council of Inspectors General on Integrity Efficiency (and its integrity committee, specifically); ensure IGs are only removed for justiciable and compelling reasons (and Congress is notified); and limit who can serve as acting IGs. There are also stipulations for notifying Congress when an agency doesn’t provide requested information or assistance to an IG and providing more training opportunities for IGs.
In an effort to address persistent watchdog job vacancies, the bill’s text states: “If the president fails to make a formal nomination for a vacant inspector general position that requires a formal nomination by the president to be filled within the period beginning on the later of the date on which the vacancy occurred or on which a nomination is rejected, withdrawn, or returned, and ending on the day that is 210 days after that date, the president shall communicate, within 30 days after the end of such period and not later than June 1 of each year thereafter, to the appropriate congressional committees.”
From the federal employee benefits front —
FedWeek gives us last minute guidance on the Federal Employee Benefits Open Season that ends next Monday December 12.
The Wall Street Journal offers ideas for use of flexible spending account dollars. The article make a point that was not on the FEHBlog’s radar screen:
This year’s December FSA spending crunch could be worse than usual. While you’re meant to empty your FSA every year, during the pandemic the government relented on this rule, allowing FSA savers to roll over what they saved in 2020 and 2021, with some accounts swelling to more than $7,000.
That special treatment is set to end in 2022, meaning if you have been accumulating money in your FSA, you may need to empty our account by Dec. 31 or you risk losing it all. “Some people might be in for a rude surprise,” says Spiegel.
Employers are permitted to give workers a little wiggle room—but not much. Some plans include a rollover provision that allows account holders to carry forward a small portion of their savings, although this amount is limited to $570 for 2022. Other plans may allow a spending grace period of up to 10 weeks.
From the infectious disease front —
The Wall Street Journal brings us up to date on Omicron treatments.
The Hill reports on the state of the flu and RSV surges. “Dr. Andrew Pekosz, a virologist and professor at Johns Hopkins Bloomberg School of Public Health, believes the U.S. is still in the “early stages” of a surge in influenza cases, he told Nexstar. * * * “With RSV we seem to be hitting a plateau,” said Pekosz. “Case numbers have not increased significantly for a couple of weeks, but they’re still at a very high level. So the burden of RSV is still great, but we may be closer to the peak there than we are with flu.”
Forbes relates, “A newly discovered immune response inside the nose could explain why respiratory illnesses like RSV, Covid, the common cold and flu thrive in winter, according to research published Tuesday in The Journal of Allergy and Clinical Immunology, a finding that challenges the conventional wisdom that infections spread because people are stuck indoors and signposts ways to develop new treatments.”
From the Rx development and coverage front
MPR informs us “The Food and Drug Administration (FDA) has granted Fast Track designation to PH10 for the treatment of major depressive disorder (MDD). * * * Results showed that treatment with PH10 significantly reduced depressive symptoms as early as 1 week based on the 17-item Hamilton Depression Scale (HAM-D-17) scores compared with placebo (P =.022). The intranasal spray was found to be well tolerated, with no serious adverse events reported.”
Touted by celebrities, raved about by TikTok users, and advertised by med spas, a new class of drugs for treating diabetes and obesity has exploded in popularity for its weight-loss effects, leading to rippling shortages across several of the medications.
Amid the surge in demand, Eli Lilly and pharmacies have started to tighten access to the latest of this type of drug, tirzepatide, focusing on giving it to people with type 2 diabetes, the only population it’s authorized for so far. But that’s left another set of patients scrambling — people with clinical obesity who turned to the medication as one of their few options for treatment. * *
There’s much overlap between the two conditions, said Beverly Tchang, an endocrinologist and assistant professor of clinical medicine at Weill Cornell Medicine. “Obesity can lead to diabetes, diabetes can lead to obesity,” she said. “They’re very much intertwined, and to treat one but not the other seems inequitable.” Tchang treats both types of patients and feels the drug shouldn’t be conserved for one group at the expense of the other.
From the telehealth front, mHealth Intelligence explains
FAIR Health’s Monthly Telehealth Regional tracker reported no change in telehealth usage in September compared with August and noted that COVID-19 fell in its rankings on top telehealth diagnoses lists in all regions and at the national level.
The FAIR Health Monthly Telehealth Regional tracker is a complimentary service that analyzes how telehealth activity and use change monthly by tracking various factors such as claim lines, procedure codes, and diagnostic categories. It represents the privately insured population, including Medicare Advantage but excluding Medicare Fee-for-Service and Medicaid beneficiaries.
MedPage Today informs us “Drug overdose deaths in pregnancy or the postpartum period increased sharply in the U.S. in recent years, with the rise most pronounced at the start of the COVID-19 pandemic in 2020, researchers reported. * * * Jacob S. Ballon, MD, MPH, of Stanford University in California, noted that the study authors did not provide explanations for why the overdose-related death rate rose sharper among the pregnant and postpartum group during the study period, but said it will likely be the basis for further research. “[It’s] an interesting signal,” said Ballon, who was not involved with the study. “But now what do we do with that to explain it or make some sense of it?”
Increased delays in discharging patients who require additional care after a hospital stay could slow their recovery, potentially harming health outcomes and quality of life, the American Hospital Association cautioned in a report released Tuesday.
The inability to discharge patients is putting additional strain on hospitals operating with thin workforces, and health systems are bearing the cost of care for patients who stay excess days without appropriate reimbursement, the AHA said.
The association has urged Congress to help offset the costs of care for patients’ additional days in the hospital by creating a temporary per diem Medicare payment targeted to acute, long-term care, rehabilitation and psychiatric facilities.
Imagine going into your doctor’s office and facing not a staff of overworked doctors and nurses, but an inviting conversation. A talk with a healthcare professional who has plenty of time, isn’t in a hurry and is ready to listen to a recital of the different aches and pains of your life. Someone with expertise in medications dedicated to making your life easier and healthier. A professional who makes and then hands you a cup of coffee before you even start talking.
With that conversation–easy, low stress–you can begin a level of trust with your doctor’s office that you might not have had before. And the person listening may, in conjunction with the doctors and nurses, find some better paths to helping you get healthier, even if you suffer from a chronic disease.
That’s the vision that Fergus Hoban has for the American healthcare system. His company, UpStream, provides integrated services for primary care physicians, both independently and as part of networks or bigger healthcare systems. Centered around a prescribing pharmacist, a team of nurses and other professionals work with doctors to provide better care for Medicare patients while at the same time lowering costs.
LHC Group and UnitedHealth Group have extended their merger agreement as the feds take a deeper look at the deal.
The agreement was extended until March 28, 2023, and the two companies now expect the merger to close in the first quarter of 2023, according to a filing with the Securities and Exchange Commission.
That the insurance giant intended to acquire LHC, a home health provider, was announced in March, and the deal is valued at about $5.4 billion. UnitedHealth said it plans to fold LHC into its Optum subsidiary as part of its provider arm, Optum Health, which is one of the country’s largest employers of physicians.
LHC Group would add 30,000 employees who provide more than 12 million home health services annually.
Health Payer Intelligence also tells us about positive provider and payer reactions to the CMS proposed rule to promote widespread use of electronic prior authorizations. As noted here yesterday, “[t]he proposed rule would require the implementation of Health Level 7 (HL7) Fast Healthcare Interoperability Resources (FHIR) standard Application Programming Interface (API) and mandates that payers have to explain the specific reason behind a prior authorization denial. Expedited prior authorizations will have to occur within 72 hours and non-urgent prior authorizations will have to be turned around in seven calendar days.”
From Capitol Hill, Roll Call reports the FY 2023 National Defense Authorization Act is expected to rescind the Defense Secretary’s 2021 Covid vaccine mandate for U.S. service members. “Congressional leaders are aiming to introduce the final compromise NDAA version as soon as Tuesday, with House floor action possible later in the week.”
From the infectious disease front —
Bloomberg Prognosis tells about a study confirming the Paxlovid rebounds have been blown out of proportion.
Pfizer has asked the Food and Drug Administration for an emergency use authorization applicable to its bivalent Omicron vaccine designed for children at least six months old and not over four years old.
The Health and Human Services Secretary has confirmed reported plans to end the mpox public health emergency when the current declaration expires at the end of January 2023. “But we won’t take our foot off the gas – we will continue to monitor the case trends closely and encourage all at-risk individuals to get a free vaccine.”
MedPage Today interviews Demetre Daskalakis, MD, MPH, the deputy coordinator of the White House Monkeypox Response Team, about the course of the illness since it erupted in the summer
Influenza hospitalizations this early in the season are higher than they have been in a decade, according to the CDC, with 14 pediatric deaths reported so far.
“Since October 1, there have already been at least 8.7 million illnesses, 78,000 hospitalizations, and 4,500 deaths from flu,” said CDC Director Rochelle Walensky, MD, MPH, on a call with reporters on Monday, held in part to kick off National Influenza Vaccination Week. * * *
This year, influenza vaccines are “well matched to the viruses currently circulating,” she added. The flu shots contain protection for two influenza A and two influenza B virus strains. Of influenza A viruses detected and subtyped this season, 79% have been A(H3N2) and 21% have been A(H1N1).
The CDC recommends influenza vaccination particularly for children, immunocompromised individuals, pregnant women, and people 65 and over.
It was not clear if the pediatric deaths reported so far this season involved unvaccinated children, but Fryhofer noted that previous data showed about 80% of influenza deaths occur in unvaccinated persons.
Pregnant women who get the flu shot also protect their newborns, who are not eligible for vaccination before they are 6 months of age, Fryhofer said. “If you’re not doing it for you, do it for your baby.”
For context, here are the flu case and death statistics from the last flu season before Covid struck, October 2019 through March 2020.
2019 – 2020 Winter CDC Fluview
3/28/20
Flu Deaths
24,000
Flu Cases
39,000,000
The flu is a highly contagious, dangerous disease.
NPR Shots offers consumer advice should they counter pharmacy shelves with a low or no supply of anti-fever drugs.
From the telehealth front, Health Leaders Media tells us
According to a survey commissioned by America’s Health Insurance Plans, almost 70% used telehealth in the past year because it’s more convenient than in-person care, and almost 80% say telehealth makes it easier to seek out care.
Almost 50% used telehealth because they were unable to make an in-person appointment, while 24% said they wanted to save money.
Some 36% used telehealth just once over the past year, while 53% used it between two and five times.
From the mental healthcare front, Health Payer Intelligence reports
CareFirst BlueCross BlueShield (CareFirst) is providing community-based organizations with nearly $8 million in grants to help improve behavioral healthcare access and quality for underserved youth.
The COVID-19 pandemic exacerbated the mental and behavioral health crisis among children, adolescents, and families. In response, CareFirst is investing in 19 community-based organizations in Maryland, Washington, DC, and Northern Virginia.
“CareFirst recognizes that behavioral health is an essential part of overall health, which includes a continuum of conditions ranging from severe mental health disorders to the emotional, psychological, and social factors that affect a person’s overall wellbeing,” Destiny-Simone Ramjohn, PhD, vice president of community health and social impact at CareFirst, said in the press release.
Kudos
From the Rx coverage front, Fierce Healthcare informs us
Express Scripts, which is part of Cigna’s Evernorth subsidiary, said Monday that it will add biosimilars for Humira to its largest formularies as preferred products available for patients with inflammatory conditions. Like other major PBMs, Express Scripts sees significant potential in biosimilars to help address the massive costs associated with specialty drugs.
Specialty drugs account for just 2% of prescriptions but drive half of drug spending.
In October 2021, Express Scripts announced that it would put Semglee, the first Food and Drug Administration-approved interchangeable insulin biosimilar, on its National Preferred Formulary for 2022. The company estimates that this move generated $20 million in savings in the first year.
From the federal government employee benefits front, Federal News Network relates
The Office of Personnel Management plans to suspend applications for the Federal Long Term Care Insurance Program for two years beginning Dec. 19, in anticipation of a sizeable rate hike.
OPM announced the unusual measure last month in the Federal Register, and noted that federal workers who submit their applications by the deadline will still be considered for enrollment. FLTCIP was created in 2002 and assists with health care costs for participants who need help with daily personal functions, or who have a severe cognitive illness, and covers home care, nursing home or assisted living benefits.
“OPM is suspending applications for coverage in FLTCIP to allow OPM and the FLTCIP carrier to assess the benefit offerings and establish sustainable premium rates that reasonably and equitably reflect the cost of the benefits provided,” the agency wrote.
The program will continue to operate normally for current enrollees, although they will not be able to apply to increase their coverage. There are currently around 267,000 federal workers and retirees participating in the insurance plan, and OPM typically receives only a few thousand applications to enroll per year.
The decision to suspend applications for the program came after John Hancock Life and Health Insurance Co., the contractor that administers the program, informed OPM that it is likely that there will a premium increase sometime next year.
Finally, the Wall Street Journal offers an interesting article about medical research that is “uncovering links between your ‘subjective age’ [as opposed to your chronological age] and your future health and longevity.”
From the Omicron and siblings front, the Centers for Disease Control’s weekly interpretative summary of its Covid statistics explains
Cases
As of November 30, 2022, the current 7-day average of weekly new cases (43,300) decreased 1.2% compared with the previous 7-day average (43,837). A total of 98,777,220 COVID-19 cases have been reported in the United States as of December 30, 2022.
Variant Proportions
CDC Nowcast projections* for the week ending December 3, 2022, estimate the proportion of lineages designated as Omicron with estimates above 1%: BA.5—and four of its sublineages (BQ.1, BQ.1.1, BF.7, and BA.5.2.6)—BA.4.6,and XBB. XBB is a recombinant of two BA.2 sublineages.
New Hospital Admissions
The current 7-day daily average for November 23–29, 2022, was 4,201. This is a 17.6% increase from the prior 7-day average (3,572) from November 16–22, 2022.
Vaccinations
As of November 30, 2022, 655.3 million vaccine doses have been administered in the United States. Overall, about 267.3 million people, or 80.5% of the total U.S. population, have received at least one dose of vaccine. About 228.4 million people, or 68.8% of the total U.S. population, have completed a primary series.
Of those who have completed a primary series, about 114.8 million people have received a booster dose,* and more than 39.7 million people have received an updated (bivalent) booster dose. But 48.3% of the total booster-eligible population has not yet received a booster dose. Learn more about who is eligible.
Deaths
The current 7-day average of new deaths (254) decreased 32.4% compared with the previous 7-day average (376). As of November 30, 2022, a total of 1,077,303 Covid-19 deaths have been reported in the United States
The CDC also released an encouraging report about Paxlovid’s efficacy.
Summary
What is already known about this topic?
Nirmatrelvir-ritonavir (Paxlovid) is an outpatient antiviral medication recommended for adults with mild-to-moderate COVID-19 who have elevated risk of severe illness.
What is added by this report?
Among U.S. adults diagnosed with COVID-19, including those with previous infection or vaccination, persons who were prescribed Paxlovid within 5 days of diagnosis had a 51% lower hospitalization rate within 30 days after diagnosis than those who were not prescribed Paxlovid.
What are the implications for public health practice?
Paxlovid should be offered to eligible adults irrespective of vaccination status, especially in groups with the highest risk for severe COVID-19 outcomes, such as older adults and those with multiple underlying health conditions.
Also from the public health front, the CDC’s Fluview tells us
Seasonal influenza activity is high and continues to increase across the country.
Of influenza A viruses detected and subtyped this season, 79% have been influenza A(H3N2) and 21% have been influenza A(H1N1).
Two influenza-associated pediatric deaths were reported this week, for a total of 14 pediatric flu deaths reported so far this season.
CDC estimates that, so far this season, there have been at least 8.7 million illnesses, 78,000 hospitalizations, and 4,500 deaths from flu.
The cumulative hospitalization rate in the FluSurv-NET system is higher than the rate observed in week 47 during every previous season since 2010-2011.
The number of flu hospital admissions reported in the HHS Protect system during week 47 almost doubled compared with week 46.
The majority of influenza viruses tested are in the same genetic subclade as and antigenically similar to the influenza viruses included in this season’s influenza vaccine.
All viruses collected and evaluated this season have been susceptible to influenza antivirals.
An annual flu vaccine is the best way to protect against flu. Vaccination helps prevent infection and can also prevent serious outcomes in people who get vaccinated but still get sick with flu.
CDC recommends that everyone ages 6 months and older get a flu vaccine annually. Now is a good time to get vaccinated if you haven’t already.
There are also prescription flu antiviral drugs that can be used to treat flu illness; those need to be started as early as possible.
The Wall Street Journal offers a helpful overview of the tripledemic situation.
Scientific meetings about Alzheimer’s disease can be funereal affairs, with researchers from around the world gathering in hopes that the latest in a long line of negative clinical trials might light the path to a long-awaited success.
This year was different. Nearly 2,000 people showed up to the Clinical Trials in Alzheimer’s Disease meeting, a conference record, to hear about lecanemab, a drug from Eisai and Biogen that appears to have broken the decades-long cycle of disappointment.
A packed audience repeatedly burst into applause during Eisai’s lecanemab presentation on Tuesday — with onlookers clapping even when they learned that the results had been concurrently published in the New England Journal of Medicine. Supplemental figures don’t usually don’t draw cheers, but the warm reception underscored how overjoyed researchers were to have any kind of success against Alzheimer’s, even a modest one. * * *
Several researchers compared this moment in Alzheimer’s research to the early days of cancer therapy or HIV treatment — the first drugs aren’t smash hits, but they’re something for scientists and doctors to build on and learn from.
“It’s not like you’ve won the war with lecanemab,” said Eric Siemers, chief medical officer of Acumen Pharma. “We’ve got a lot of work to do. But this is an inflection point. There’s no question about it.”
In that regard, BioPharma Dive points out lessons learned from testing a Roche drug similar to lecanermab.
After one year of treatment, [the Roche drug] gantenerumab reduced amyloid burden in patients only half as well as the trials’ designers had expected based on previous research, said researcher Randall Bateman, a neurology professor at Washington University in St. Louis who helped lead the studies.
Moreover, around half as many gantenerumab patients as predicted tested negative for amyloid over the course of the trial. Almost none tested negative after one year of treatment, and only around a quarter did after more than two years, researchers revealed.
Data for lecanemab and donanemab presented at CTAD, meanwhile, showed stronger amyloid clearance, helping boost confidence in those drugs.
Bateman also pointed to a post-study analysis researchers conducted of Roche’s trials that hinted at better outcomes for trial participants who had higher reductions in amyloid, although this finding wasn’t statistically conclusive.
Taken together with data from other trials, gantenerumab’s results should help researchers as they try to optimize available therapies and develop new ones, Bateman said.
“I see this as one of the missing essential pieces of the puzzle of figuring out how to optimally treat along this pathway for amyloid removal,” he said.
Meanwhile, the New York Times tells us about “A Promising Trial Targets a Genetic Risk for Alzheimer’s Preliminary results offer hope that gene therapy can protect people with a version of the brain disease driven by a particular gene variant.”
From the U.S. healthcare business front, Healthcare Dive reports
Advocate Aurora Health and Atrium Health announced Friday the two providers have closed their merger deal, becoming the nation’s fifth-largest nonprofit health system by revenue.
The new system, Advocate Health, will generate revenue of more than $27 billion and operate 67 hospitals and more than 1,000 sites of care in six states. The system expects to treat nearly 6 million patients each year. * * *
Instead, economists told Healthcare Dive, the FTC is likely to examine insurer overlap in the case of Advocate Health. The combined entity operates in Illinois, Wisconsin, Georgia, North Carolina, South Carolina and Alabama.
The Biden administration will allow agencies to hire employees in certain positions on a temporary basis for up to 10 years, more than doubling the current cap limiting the assignments for those workers.
The Office of Personnel Management issued the rule on Thursday, finalizing a proposal first put forward by the Trump administration. The rule will enable federal agencies to appoint employees in STEM jobs for a decade. OPM said the change would give agencies more flexibility when tackling long-term science, technology, engineering and mathematics projects. Previous regulations required agencies to get special permission from OPM to keep any term employee on staff for longer than four years.
Viet Tran, an OPM spokesman, said the rule showed the administration’s “commitment to STEM hiring.” He added it would allow for more federal, rather than outsourced, hiring.
“With this final rule, agencies have more flexibility and support (and less administrative burden) to hire employees—rather than contractors—for non-permanent STEM positions that agencies expect from the outset to last longer than 4 years but not more than 10 years,” Tran said. “This is another tool to help agencies better compete for talent.”
As the FEHBlog has explained, federal employees can expect a 4.6% pay raise for 2023 with 4.1% of the increase being distributed across the GS schedule and the remaining 0.5% allocated to locality pay. As it turns out, the Society for Human Resource Management tells us
Employers in the U.S. plan to boost salaries an average of 4.6 percent in 2023, up from 4.2 percent this year, according to a new study.
Employers say inflationary pressures and the ongoing challenges of finding and keeping workers are the main reasons for the higher projected increases. Indeed, 3 in 4 of the 1,550 U.S. employers in the latest Salary Budget Planning Report by consultancy WTW say they continue to experience problems attracting and retaining workers.The survey was conducted from Oct. 3 to Nov. 4, 2022.
From the plan design front, a recent Kaiser Family Foundation report explains the growing use of all sizes of employers to provide retiree health benefits through Medicare Advantage plans.
This analysis uses data from the 2022 KFF Employer Health Benefits Survey to examine the extent to which large private and non-federal public employers that offer retiree health benefits are turning to Medicare Advantage and why they are making this shift. However, the Survey does not include information about union-administered benefits. For additional information about methods, see Survey Design and Methods.
Based on the Survey, we find:
Half (50%) of large employers offering retiree health benefits to Medicare-age retirees offer coverage to at least some retirees through a contract with a Medicare Advantage plan, nearly double the share in 2017 (26%).
About 44% of large employers that offer Medicare Advantage coverage to their retirees do not give retirees a choice in coverage options.
Among larger employers with 1,000 or more workers that offer retiree health benefits through a Medicare Advantage plan, the most commonly cited reason they elected this option was the lower cost.
FEHB plans also are implementing integrated Medicare Advantage plans as a cost-saving measure.
From the HHS front, “Today, the U.S. Department of Health and Human Services (HHS) Secretary Xavier Becerra marked the one-year anniversary of HHS’s Overdose Prevention Strategy (Strategy) by announcing the progress the nation has made since the release of the Strategy, showing expanded treatment capacity, lives saved from an overdose, and commitment to long term recovery supports.” Kudos. Here is the fact sheet.
We use cookies on our website to give you the most relevant experience by remembering your preferences and repeat visits. By clicking “Accept”, you consent to the use of ALL the cookies.
This website uses cookies to improve your experience while you navigate through the website. Out of these, the cookies that are categorized as necessary are stored on your browser as they are essential for the working of basic functionalities of the ...
Necessary cookies are absolutely essential for the website to function properly. These cookies ensure basic functionalities and security features of the website, anonymously.
Cookie
Duration
Description
cookielawinfo-checbox-analytics
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Analytics".
cookielawinfo-checbox-functional
11 months
The cookie is set by GDPR cookie consent to record the user consent for the cookies in the category "Functional".
cookielawinfo-checbox-others
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Other.
cookielawinfo-checkbox-necessary
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookies is used to store the user consent for the cookies in the category "Necessary".
cookielawinfo-checkbox-performance
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Performance".
viewed_cookie_policy
11 months
The cookie is set by the GDPR Cookie Consent plugin and is used to store whether or not user has consented to the use of cookies. It does not store any personal data.
Functional cookies help to perform certain functionalities like sharing the content of the website on social media platforms, collect feedbacks, and other third-party features.
Performance cookies are used to understand and analyze the key performance indexes of the website which helps in delivering a better user experience for the visitors.
Analytical cookies are used to understand how visitors interact with the website. These cookies help provide information on metrics the number of visitors, bounce rate, traffic source, etc.
Advertisement cookies are used to provide visitors with relevant ads and marketing campaigns. These cookies track visitors across websites and collect information to provide customized ads.